CHAPTER 7 Hip Instability
Unlike the shoulder, which relies primarily on static and dynamic soft tissue restraints for its stability, the hip depends primarily on its osseous anatomy. The hip’s unique soft tissue envelope also plays a role in its stability, particularly when there is any significant deviation from normal.1 When considering a patient with hip pain that is believed to be at least in some way the result of hip instability, both osseous and soft tissue constraints must be considered. Traumatic dislocation is typically accompanied by a history of an acute event. Atraumatic hip instability can result from repetitive rotational movements. The hypothesized mechanism for this type of instability is a subclinical capsular laxity accompanied by mild hip dysplasia that may progress over time.2 Generalized laxity and connective tissue disorders are also causes of atraumatic instability.
ANATOMY
Although relying largely on its bony anatomy, hip stability is complemented by the acetabular labrum and capsuloligamentous complex. In the neutral anatomic position, the anterior part of the femoral head is not engaged in the acetabulum. The acetabular labrum compensates for this by covering this portion of the femoral head. The labrum is attached to the transverse acetabular ligament anteriorly and posteriorly at the base of the fovea and proceeds to run around the circumference of the acetabular rim.1 The labrum deepens the “socket” and aids in maintaining the suction effect that provides additional hip stability. Absence of the labrum can lead to a loss of this suction effect, as well as increased cartilage surface consolidation as a result of the loss of hydration, thereby increasing contact pressures.3–5 Proprioceptors and nociceptors have been identified within the labrum and may explain the decreased proprioception and increased pain in the athlete with a torn labrum.6 Much like the meniscus in the knee, the labrum is largely avascular, except for the most peripheral portion near the capsule, limiting its ability to heal.7
The labrum is not, however, a stand-alone structure. It functions in conjunction with the capsuloligamentous complex. The fibrous hip capsule and its ligaments are like a thick sleeve. Anteriorly, this complex primarily consists of the iliofemoral ligament (ligament of Bigelow), a 12- to 14-mm thick structure shaped like an inverted Y. It provides resistance to hip extension beyond neutral and resists external rotation. The pubofemoral ligament, which arises from the pubic portion of the acetabular rim and passes below the neck of the femur to blend with the most inferior fibers of the iliofemoral ligament, reinforces the inferior and anterior capsules, resisting extension and abduction. The ischiofemoral ligament reinforces the posterior surface of the capsule and has a spiraling pattern. Finally, the zona orbicularis is a deep layer of fibers within the capsule that forms a circular pattern around the femoral neck, constricting the capsule and helping maintain the femoral head within the acetabulum.1
The position of maximum hip joint stability is in full extension because it is in this position that the twisted orientation of the capsular ligaments causes a screw-home effect.1 However, the articular surfaces of the hip joint are not in optimal contact in this position (the close-packed position). Optimal contact occurs in the loose packed position of flexion and lateral rotation as the ligaments uncoil. The greatest risk of traumatic dislocation, then, is when the joint is between the close-packed and maximally congruent position (flexed and adducted position). The ligamentum teres and psoas tendon are two extra-articular structures about the hip that deserve additional discussion. The ligamentum has no real stabilizing effect on the joint, whereas the psoas protects the anterior intermediate capsule, which is devoid of ligamentous protection.
CLINICAL EVALUATION
History
Making the diagnosis of hip instability can be a diagnostic dilemma. Hip instability can manifest as overtly as frank traumatic dislocation or can be as obscure as occult groin pain or clicking. Hip pain, clicking, or “giving way” in the young adult patient may arise from any number of anatomic structures. The picture can be further complicated by referred pain from the lumbosacral region as well as the genitourinary tract and abdominal wall.8 Age also plays a significant role in determining a differential diagnosis for hip pain.9 In children, hip dislocation, bony avulsions, apophyseal injuries, fractures, slipped capital femoral epiphysis (SCFE), Legg-Perthes disease, developmental dysplasia of the hip (DDH), and toxic and septic arthritis are all potential causes.9
Physical Examination
Antalgic gait patterns in which there is shortening of the stance phase and step length on the affected side can result from instability. A Trendelenburg gait may indicate an attempt to bring the center of gravity over the affected side to decrease the moment arm across that hip joint.10 The patient with atraumatic instability may be able to demonstrate subluxation or dislocation of the involved hip, although this is rare.
Traumatic hip instability can manifest with pain on prone extension–external rotation of the involved hip. A positive axial distraction test can be confirmed with a positive vacuum sign on dynamic fluoroscopy (Fig. 7-1).1 Anterior apprehension may also be elicited with the patient in the lateral decubitus position while suspending the affected leg in slight abduction (Fig. 7-2). The presence of a positive examination indicates capsular laxity in traumatic and atraumatic instability.


FIGURE 7-2 Apprehension position. The patient is placed in the lateral decubitus position and the affected extremity is supported by the examiner. The examiner uses the other arm to push the hip in an anterior direction as pressure is applied over the posterior aspect of the greater trochanter. In symptomatic patients, a sensation of subluxation can sometimes be elicited, whereas in others, there is a reproduction of their pain.
In some patients, and with proper relaxation, a sense of the end range of capsular tightness and the end point of the ligamentum teres can be obtained by the supine external rotation test, in which the patient is placed supine and the affected leg is suspended in 30 degrees of flexion by the examiner. With gentle external rotation, while the patient is relaxed, the end point of external rotation can be assessed (Fig. 7-3). Also, a comparison can be made with the contralateral (and presumably normal) extremity. If there is a significant increase in external rotation as compared with the normal extremity, laxity of the Y ligament can be inferred. Also, if a large anterior labral tear exists, audible snapping and reproduction of pain can be elicited.

IMAGING
Several radiographic indices have been described to differentiate normal from abnormal osseous anatomy based on the AP pelvic radiograph. The Tonnis angle is used to assess lateral subluxation of the femoral head and subsequent increased forces across the weight-bearing acetabulum (Fig. 7-4).11 A measurement of less than 10 degrees is considered normal.
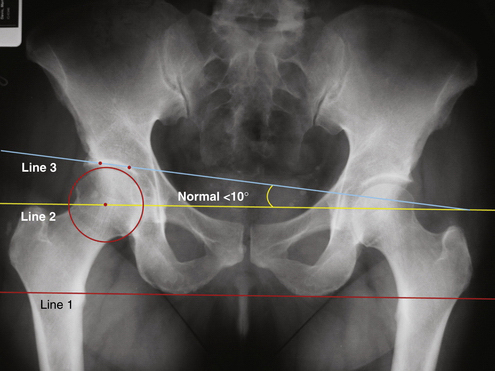
FIGURE 7-4 AP radiograph showing the technique of measuring the Tonnis angle (normal, <10 degrees). In this case, the red line (line 1) connecting the two ischial tuberosities is the reference line on which all other lines are based. The yellow line (line 2) is a line drawn parallel to line 1 through the center of the femoral head. The angle formed between line 2 and a third line connecting two points demarcating the sourcil or weight-bearing surface of the acetabulum is the Tonnis angle.
(Adapted from Delaney S, Dussault RG, Kaplan PA, et al. Radiographic measurements of dysplastic adult hips. Skeletal Radiol. 1997;26:75-81.)
The center edge angle of Wiberg assesses acetabular inclination (Fig. 7-5). This angle should measure at least 20 to 25 degrees to be considered normal.12,13 One can estimate acetabular version using the AP pelvis by looking for a crossover sign (Fig. 7-6). The two lines involved estimate the posterior and anterior rims of the acetabulum. The posterior rim is traced from the ischial tuberosity superolaterally to the roof of the acetabulum. The anterior rim is traced from the teardrop in a superior and lateral direction along the rim to the roof. If these lines cross, it is estimated that the acetabulum is retroverted; if not, it is assumed that the acetabular version is within the normal 10- to 15-degree anterior version.14,15
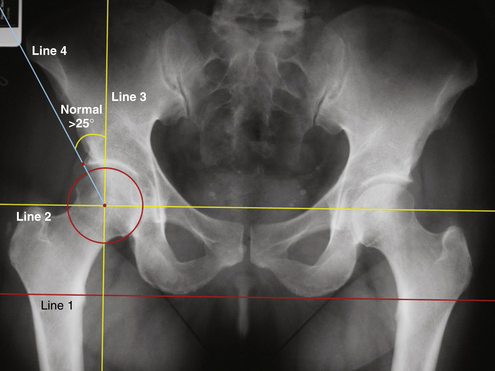
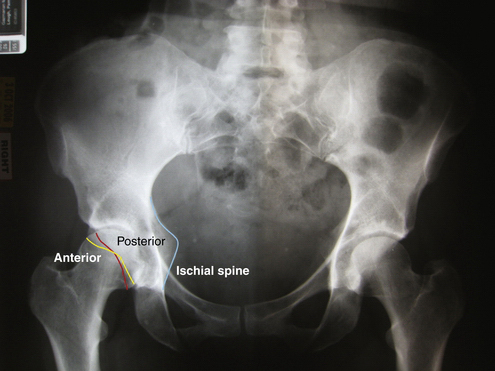
FIGURE 7-6 AP radiograph demonstrating the crossover sign indicating acetabular retroversion. Note that the red line (representing the anterior wall of the acetabulum) crosses the yellow line (representing the posterior wall of the acetabulum). Also of note is the visualization of the ischial tuberosity (blue line), which is normally superimposed by the acetabulum, but easily visible in the retroverted acetabulum.
When evaluating a patient with potential residual dysplasia, the faux profile view is often used to evaluate anterior and lateral coverage of the femoral head by the acetabulum. Although plain radiographs are sufficient for diagnosis in a number of cases, there are pathologic entities that require further investigation. Imaging of bony lesions about the hip is best accomplished using computed tomography (CT) because it provides the greatest spatial resolution of bony structures. Cases of questionable hip dysplasia should use CT in preoperative planning. The use of intra-articular contrast in CT arthrography can increase the contrast between cartilage and labral tissue.8
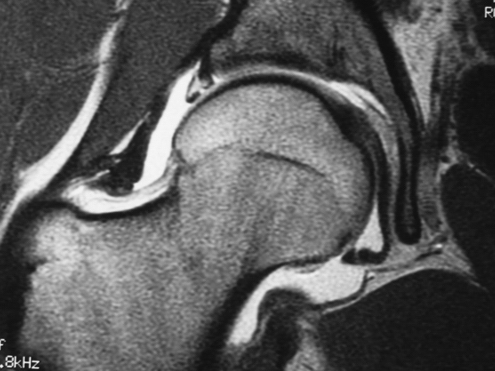
Magnetic resonance imaging (MRI) has become the most reliable means of diagnosing unresolved hip pathology in addition to direct visualization and is often useful in cases of instability. MRI has been shown to demonstrate inflammatory arthropathies and joint effusions effectively, but has been less accurate in assessing articular cartilage lesions.8,16,17 Contrast MRI studies in patients with a torn labrum or torn iliofemoral ligament can result in a larger volume of intra-articular contrast, and thus indirectly confirm the diagnosis of instability (Fig. 7-7).1