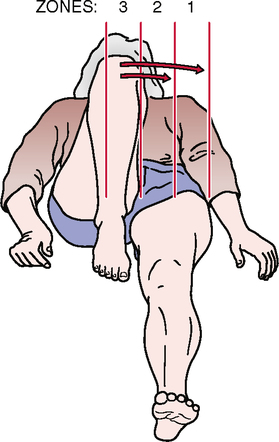
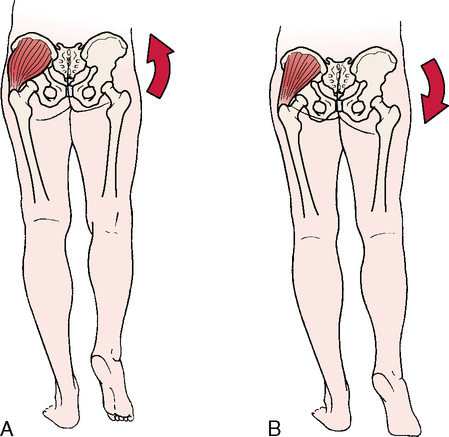
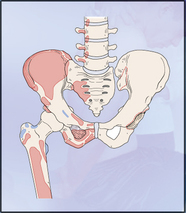
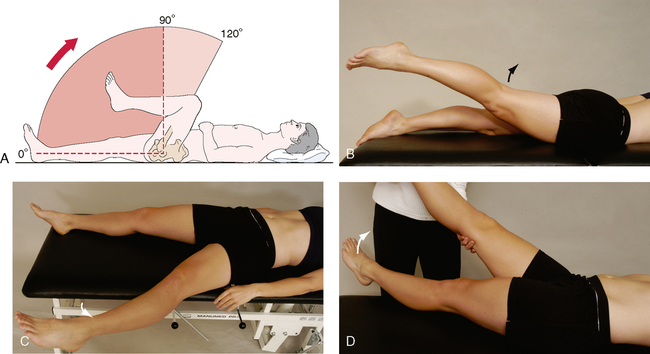
CHAPTER 10 The active movements of the hip are performed with the most painful ones being done last. Some movements are done with the patient supine and some with the patient prone. If the history indicates that repetitive movements, sustained postures, or combined movements have caused symptoms, the examiner should make sure these movements are tested as well. For example, sustained extension of the hip may provoke gluteal pain in the presence of claudication in the common or internal iliac artery.1 • During the movement, if the abdominals are weak, the pelvis will rotate anteriorly. If the hip flexors are weak, the pelvis will rotate posteriorly. • If sharp groin pain is elicited on flexion and medial rotation (combined movement), the pain may be the result of anterior impingement of the femoral neck against the acetabular rim.2–6 In the supine position, the patient simply rotates the straight leg on a balanced pelvis. Turning the foot or leg outward tests lateral rotation; turning the foot or leg inward tests medial rotation. The examiner can then measure hip rotation by having the patient hold the foot in plantigrade and measuring the angle of the foot to a vertical line from the middle of the heel. In another supine test, the patient is asked to flex both the hip and knee to 90º, as the patient would do when tested in sitting.7 When this method is used, it must be recognized that having the patient rotate the leg outward tests medial rotation, whereas having the patient rotate the leg inward tests lateral rotation. Patrick’s test (flexion, abduction, and external rotation [FABER] or figure-four test) Anterior labral tear test (flexion, adduction, and internal rotation [FADDIR] test) • Osteoarthritis affects 10% to 25% of the population over age 55. • Osteonecrosis can occur in people of any age, but it is most common in people in their 30s, 40s, and 50s. • In children, the most common cause of hip pain is acute transient synovitis. The incidence of slipped capital femoral epiphysis is about 6.1 per 10,000 in boys and 3 per 10,000 in girls. The incidence of Leg!g-Calvé-Perthes disease is about 1.5 to 5 per 10,000. • In newborns, the prevalence of developmental dysplasia of the hip (DDH) has been reported in screened populations at rates of 2.5 to 20 per 1000 births; however, it reaches 40 to 90 per 1000 births in some communities. PATRICK’S TEST (FLEXION, ABDUCTION, AND EXTERNAL ROTATION [FABER] OR FIGURE-FOUR TEST)14–16
HIP
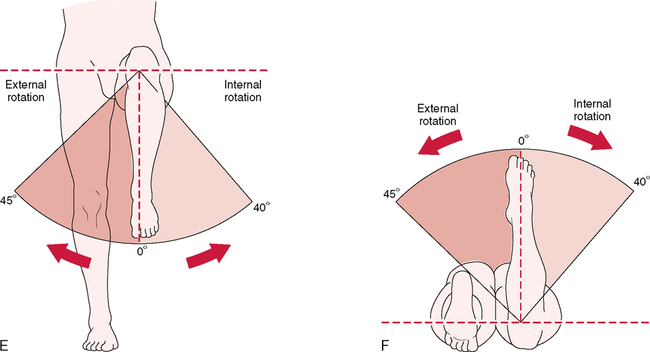
SELECTED MOVEMENTS
SPECIAL TESTS FOR HIP PATHOLOGY8–13
Relevant Special Tests
Epidemiology and Demographics
Mechanism of Injury