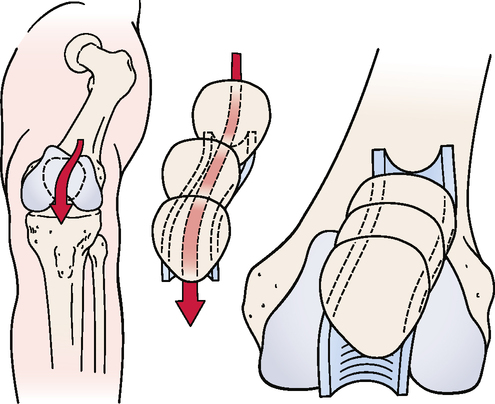
CHAPTER 11 • When the patella is pushed medially or laterally, the examiner should note whether it stays parallel to the femoral condyles or tilts or rotates. For example, if the patella is pushed medially when the medial structures are tight, the lateral border of the patella tilts up. Likewise, with tight lateral structures, the medial border tilts up. If the lateral structures are tight superiorly, the inferior pole of the patella medially rotates. These are examples of dynamic tilt and rotation problems of the patella. • Mild to moderate knee pain is present. • The patient reports feeling a tearing in the knee, not a “pop.” • Bruising in the medial knee often is present, because the MCL/TCL is an extra-articular structure. • Swelling builds up slowly over several days. • The patient walks with a limp and has pain on knee extension, because extension stretches the ligament. • Instability and “giving way” may be noted. • Loss of knee motion and moderate stiffness may be present. • Medial joint line pain or pain where the ligament attaches to the femur or tibia may be reported. Avulsion of ligaments generally occurs between the unmineralized and mineralized fibrocartilage layers. MCL/TCL injury occurs most often at the femoral attachment (65% of cases).6–11 ABDUCTION (VALGUS STRESS) TEST12,13 • A positive test result on full extension is classified as a major disruption of the knee. The examiner usually finds that one or more of the rotary tests also produce a positive result. • If the examiner applies lateral rotation to the foot when performing the test in extension and finds excessive lateral rotation on the affected side, this is a sign of possible anteromedial rotary instability. • The flexed part of the valgus stress test is considered the true test for one-plane medial instability, because the cruciates are eliminated. Injury to the LCL/FCL is the least common knee ligament injury. Injuries to the LCL/FCL are rare, accounting for only 2% of all knee injuries. The LCL/FCL is the least likely knee ligament to be sprained, because most LCL/FCL injuries are caused by a blow to the inside of the knee, and that area usually is shielded by the opposite leg.6,7,9–11 • Mild to moderate knee pain is present. • The patient may report feeling a pop in the knee. • Loss of knee motion and moderate stiffness are present. • Lateral joint line pain may be reported. • Bruising in the lateral knee often is present, because the LCL/FCL is an extra-articular structure. • Swelling builds up slowly over several days.
KNEE
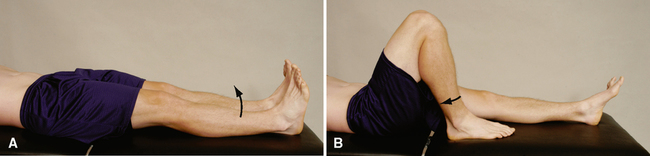
SELECTED MOVEMENTS
SPECIAL TESTS FOR ONE-PLANE MEDIAL INSTABILITY
Relevant Special Tests
Relevant Signs and Symptoms
Mechanism of Injury


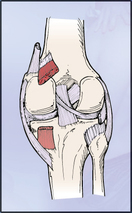
SPECIAL TESTS FOR ONE-PLANE LATERAL INSTABILITY
Relevant Special Tests
Epidemiology and Demographics
Relevant Signs and Symptoms
KNEE