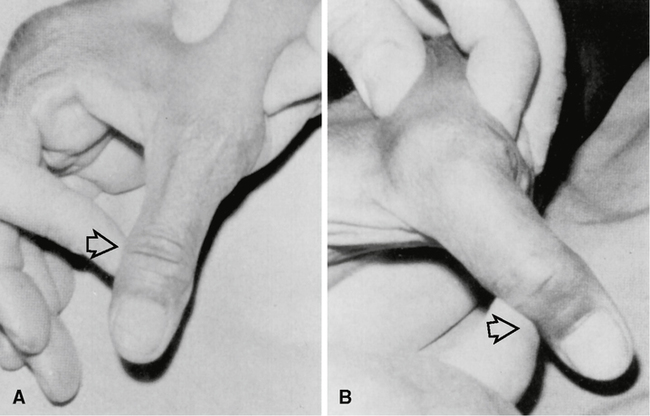
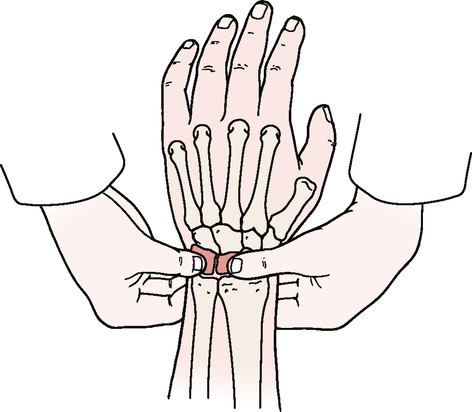
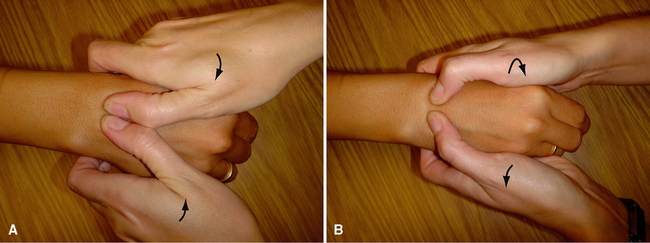
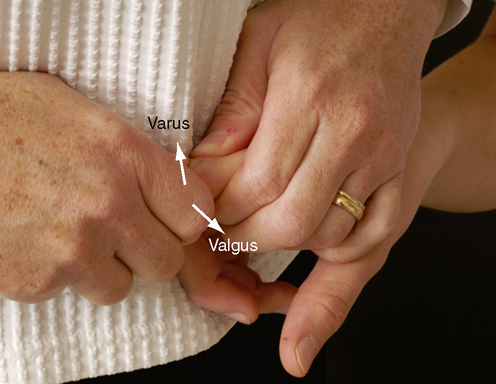
CHAPTER 6 INDICATIONS OF A POSITIVE TEST Pronation and supination. Active pronation and supination of the forearm and wrist are approximately 85° to 90°, although this varies from individual to individual. It is more important to compare the movement with that of the normal side. Approximately 75° of supination or pronation occurs in the forearm articulations. The remaining 15° is the result of wrist action. Wrist flexion and extension. Wrist flexion is 80° to 90°; wrist extension is 70° to 90°. The end feel of each movement is tissue stretch. Radial and ulnar deviation. Radial and ulnar deviations of the wrist are 15° and 30° to 45°, respectively. The normal end feel of these movements is bone to bone. Finger flexion. Flexion of the fingers occurs at the metacarpophalangeal joints (85° to 90°), followed by the proximal interphalangeal joints (100° to 115°) and the distal interphalangeal joints (80° to 90°). Finger extension. Extension occurs at the metacarpophalangeal joints (30° to 45°), the proximal interphalangeal joints (0°), and the distal interphalangeal joints (20°). The end feel of finger flexion and extension is tissue stretch. Finger abduction and adduction. Finger abduction occurs at the metacarpophalangeal joints (20° to 30°); the end feel is tissue stretch. Finger adduction (0°) occurs at the same joint. Thumb flexion. Thumb flexion occurs at the carpometacarpal joint (45° to 50°), the metacarpophalangeal joint (50° to 55°), and the interphalangeal joint (80° to 90°). It is associated with medial rotation of the thumb as a result of the saddle shape of the carpometacarpal joint. Thumb extension. Extension of the thumb occurs at the interphalangeal joint (0° to 5°); it is associated with lateral rotation. Flexion and extension take place in a plane parallel to the palm of the hand. Thumb abduction and adduction. Thumb abduction is 60° to 70°; thumb adduction is 30°. These movements occur in a plane at right angles to the flexion-extension plane. • Pathological conditions in structures other than the joint may restrict ROM (e.g., muscle spasm, tight ligaments/capsules). If the examiner suspects a problem with these structures, passive movement end feels will help differentiate the problem. • Most functional activities of the hand require the fingers and thumb to open at least 5 cm (2 inches), and the fingers should be able to flex within 1 to 2 cm (0.4 to 0.8 inches) of the distal palmar crease. • If the patient complains of pain on supination, the examiner can differentiate between the distal radioulnar joint and the radiocarpal joints by passively supinating the ulna on the radius with no stress on the radiocarpal joint. If this passive movement is painful, the problem is in the distal radioulnar joint, not the radiocarpal joints. The normal end feel of both movements is tissue stretch, although in thin patients, the end feel of pronation may be bone to bone. • Wrist flexion decreases as the fingers are flexed, just as finger flexion decreases as the wrist flexes, and movements of flexion and extension are limited, usually by the antagonistic muscles and ligaments. • The digits are medially deviated slightly in relation to the metacarpal bones. When the fingers are flexed, they should point toward the scaphoid tubercle. In addition, the metacarpals are at an angle to each other. Ligamentous instability test for the fingers Thumb ulnar collateral ligament laxity or instability test Lunotriquetral ballottement (Reagan’s) test • Localized pain may occur over the injured tissue, especially when the individual is gripping, using the hand, or weight bearing on the hand. • Generalized pain may be present. • Swelling may or may not be present. • Clicking or catching may be noted with functional use. • The patient may complain of weakness in the hand and wrist. LIGAMENTOUS INSTABILITY TEST FOR THE FINGERS THUMB ULNAR COLLATERAL LIGAMENT LAXITY OR INSTABILITY TEST6,7 LUNOTRIQUETRAL BALLOTTEMENT (REAGAN’S) TEST8–10
FOREARM, WRIST, AND HAND

SELECTED MOVEMENTS
SPECIAL TESTS FOR LIGAMENT, CAPSULE, AND JONT INSTABILITY2–5
Relevant Special Tests
Suspected Injury
Relevant Signs and Symptoms
Mechanism of Injury