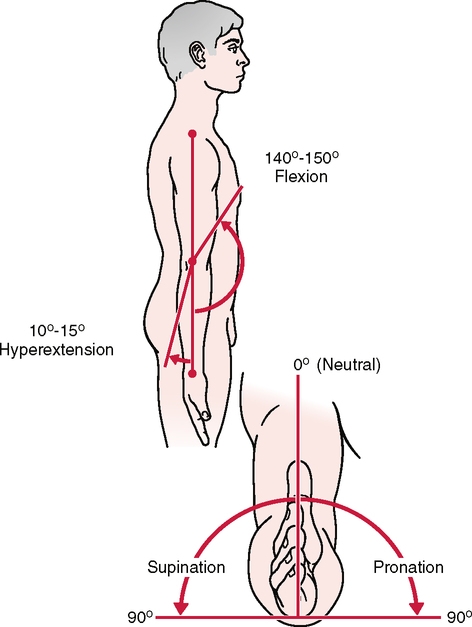
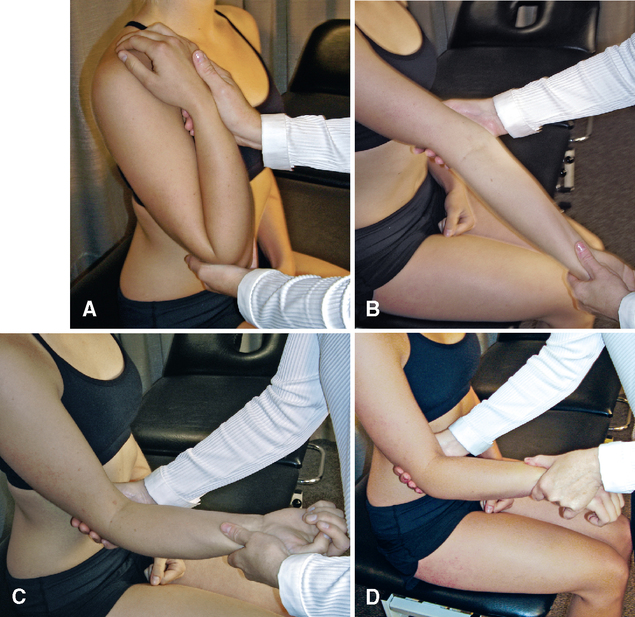
CHAPTER 5 • The examiner should test active flexion in a neutral position as well as in the fully pronated and supinated positions. Differences in flexion ROM should be noted. • Terminal flexion loss is more disabling than the same degree of terminal extension loss, because flexion is needed for so many activities of daily living. Loss of either motion affects the reach of the hand, which in turn affects function. • Normally, the extension movement is arrested by the locking of the olecranon process of the ulna into the olecranon fossa of the humerus. Loss of elbow extension is a sensitive indicator of an intra-articular pathological condition. It is the first movement lost after injury to the elbow and the first regained with healing. • The examiner should make sure the patient does not abduct the shoulder in an attempt to increase the amount of pronation or to compensate for a lack of sufficient pronation. • For both supination and pronation, only about 75° of movement occurs in the forearm articulations; the remaining 15° is the result of wrist action. • The examiner should make sure the patient’s shoulder does not adduct further in an attempt to give the appearance of increased supination or to compensate for a lack of sufficient supination. • Loss of ROM with supination often is the result of wrist injuries or fracture. Therefore, loss of motion or symptom reproduction with supination does not always imply a pathological condition of the elbow. • If the patient history includes a complaint that combined movements, repetitive movements, or sustained positions cause pain, these specific movements should be included in the active movement assessment. • Passive movements should be carried out carefully to test the end feel and to test for a capsular pattern. Tissue approximation is the normal end feel of elbow flexion; in thin patients, the end feel may be bone to bone as a result of the coronoid process of the ulna hitting in the coronoid fossa of the humerus. Pronation also may be bone to bone in thin individuals. The examiner should note whether a capsular pattern is present. • The capsular pattern for the elbow complex as a whole is more limitation of flexion than extension. RESISTED ISOMETRIC MOVEMENTS3,4 Elbow flexion. The examiner places the palm of his or her hand on the superior aspect of the patient’s forearm to provide resistance. Elbow extension. The examiner places the palm of his or her hand on the inferior aspect of the patient’s forearm to provide resistance. Pronation. The examiner grasps the patient’s forearm to provide resistance. Supination. The examiner grasps the patient’s forearm to provide resistance. Wrist flexion. The examiner holds the patient’s palm with one hand to provide resistance while stabilizing the forearm with the other. Wrist extension. The examiner holds the dorsum of the patient’s hand with one hand to provide resistance while stabilizing the forearm with the other. • If the patient has complained that combined movements under load, repetitive movements under load, or sustained positions under load cause pain, the examiner should carefully examine these resisted isometric movements and positions as well, but only after the basic movements have been tested isometrically. • Muscle flexion power around the elbow is greatest in the range of 90° to 110° with the forearm supinated. At 45° and 135°, flexion power is only 75% of maximum. • Research shows that men isometrically are two times stronger than women when testing elbow strength. In both men and women, extension is 60% of flexion and pronation is about 85% of supination. • If the history indicates that concentric, eccentric, or econcentric movements have caused symptoms, these movements should also be tested with load or no load as required. Ligamentous valgus instability test Ligamentous varus instability test Posterolateral rotary drawer test Patients may or may not have a prior history of damage to the elbow. Lateral instability occurs after elbow dislocation in 75% of cases.13 Athletes who participate in overhead sports may have a history of lower extremity or back pain that does not allow normal throwing mechanics. This can lead to excessive stress in the elbow, especially on the medial collateral ligament.
ELBOW
SELECTED MOVEMENTS


SPECIAL TESTS FOR LIGAMENTOUS INSTABILITY
Relevant Special Tests
Relevant History
Mechanism of Injury
Dislocation/Subluxation