3
High-Pressure Injection Injuries
Kevin D. Plancher
History and Clinical Presentation
A 28-year-old, right hand dominant man presented with an injury to the left hand. The patient was operating a high-pressure paint gun and tried to clear the nozzle with his free hand during operation of the equipment. The patient wiped the jet opening of the high-pressure gun with his left index finger when the gun discharged into his palm, producing a pressure of 5000 psi.
Physical Examination
The paint stream struck the palm with such pressure that the liquid penetrated the skin and spread widely throughout the underlying fascial planes and tendon sheaths. To assess the severity of the injury, the type of injected material and the time of the injection were determined. Circulation surrounding the injury was assessed by observing the general skin color and temperature and capillary refill. To confirm dual circulation to hands and fingers, the Allen’s test was performed (Fig. 3–1). Anterior forearm compartment was evaluated by passive wrist and finger extension. Distention of the tissue and the resulting inflammatory reaction caused marked ischemia of the tissue. Treatment was not delayed to avoid tissue necrosis, fever, and leukocytosis.
PEARLS
- The time between the injection and treatment may determine the severity and treatment of the injury (less than 24 hours essential).
- Tissues that survive the initial injection injury but still contain grease, paint, or oil heal slowly and may develop multiple oleogranulomas of varying sizes.
- In time, the oleomas drain through sinuses or open directly through the skin
- Wide open incision and debridement; do not try for cosmesis because of high risk for loss of digit or hand
PITFALLS
- The appearance of the wound does not determine the severity of the injury.
- Amputation is more likely if debridement is delayed more than 10 hours, especially with low viscosity substances.
- Without diagnosis and treatment, a compartment syndrome with subsequent necrosis usually destroys tissue viability.
- Do not use small openings for debridement.
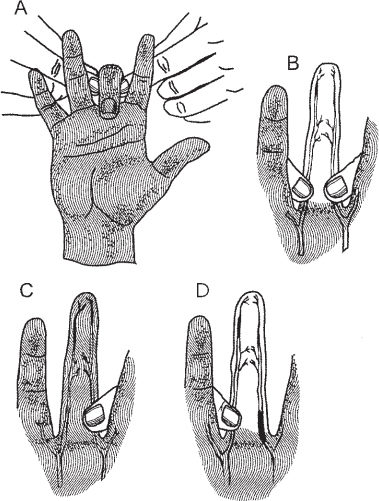
Figure 3–1.(A–D) Demonstration of digital Allen’s test to confirm circulation of fingers.
Diagnostic Studies
Standard preoperative laboratories are performed. Radiographs can be used to determine any associated fractures. Preoperative roentgenograms can assist in determining the surgical strategy by identifying subcutaneous air, debris, or unanticipated fractures.
Differential Diagnosis
Bites
Puncture wounds
Diagnosis
High-Pressure Injection Injury to the Palm
The index finger is the most frequently injured digit, followed by the palm and long finger (Fig. 3–2). If the patient delays treatment, the digit may appear erythematous or cold, edema and intense pain may develop, and loss of digit is ensured. Injuries to the digits are often associated with more morbidity than those to the hand because of potential for development of compartmental syndrome. The severity of the injury is first diagnosed by the type of fluid. Injection injuries with grease guns result in ischemia and chemical irritation, but inflammation is less severe than with paint injuries. The highest risk of early tissue necrosis and gangrene are seen with injuries involving paint, paint solvent, and paint thinner. Other fluids such as grease, oil, and other mechanical fluids may cause no reaction during the first 48 hours following the injection. However, fibrosis, oligogranuloma formation, and draining sinuses may occur. The amount of fluid injected determines the degree of vascular compression. Large volumes of fluids are associated with increased vascular compression. If the fluid was at high pressure, the result is an extension of the fluid penetration, and this may result in a larger area of spread of the injected material. Timely diagnosis and treatment are the most important factors, as the risk of amputation increases as the time from injury to treatment increases.










