There are only a few studies that have scientifically tested preventive measures in gymnastics. Additionally, to date, no studies have examined factors that impact the likelihood of a prevention strategy being adopted by the gymnastics community (i.e., translational research). However, studies in other sports have shown that it is difficult to implement injury prevention programs unless the extra practice also adds a quality or improved performance to the sport itself. The fact that the prevention programs may reduce the amount of injuries does not seem to be enough. One reason may be that prevention programs are time consuming, and to be effective should be implemented before injury—when it actually does not seem to be needed. A change in behavior must therefore be achieved. If the prevention programs are considered ordinary training and not extra training, this may be accomplished. With respect to what is known about learning and behavior we believe that prevention programs should be implemented from a young age. The prevention programs should be regarded as recovery and reactivation of the neuromuscular system and the body control, essential for the performance, not as extra practice. Since there are few studies regarding prevention of injury in gymnastics, recommendations in this chapter are in some cases drawn and presented from studies carried out in other sports.
Intrinsic strategies
Specific balance and agility training, joint stability and neuromuscular exercises, plyometric strength training as well as general strength, and stretching exercises are included in successful prevention programs in sports such as soccer and European team handball (Schiff et al., 2010). These preventive measures are also included in ordinary gymnastics training, and several of the exercises, used in prevention programs, originate from gymnastics. The neuromuscular control has to be working properly in order to avoid injury and since gymnasts spend a tremendous amount of time in practice, fatigue leading to decreased neuromuscular control may be a problem. Consequently, effective recovery of the neuromuscular control system would be one means of prevention. This may be achieved by rest, proper nutrition, and neuromuscular control exercises such as joint stability training and basic balance and agility training.
Joint stability
The stability of a joint depends on active as well as passive structures such as the joint capsule, ligaments, and deep stabilizing muscles. These structures provide joint stiffness while large force-producing muscles enable movements. The demands on each and every structure are high in gymnastics, especially since gymnasts are strong and at the same time flexible. Gymnasts practice to perfection, which means that they spend several hours repeating and practicing a skill. Although it may seem as if the muscles and the neuromuscular control system work properly there is a risk of fatigue in the deep stabilizing system. Decreased neuromuscular control of the deep stabilizing muscles may finally lead to functional joint instability, delayed muscle onset, pain, and severe injury. The importance of a well-working muscle system is obvious for a gymnast and stabilizing muscles of the joints do not seem to recover without specific activation. Therefore, a program including low-intensity specific exercises may help the recovery and prevent more severe injuries to occur. Since warm-up is part of the preparation of a gymnast, these exercises would preferably be implemented in the warm-up and target one or more joints. Balance boards, elastic bands, and gym balls as well as ordinary gymnastics equipment may be fun and helpful tools in this practice. There are several books and scientific articles presenting specific exercises for strengthening the core and joints such as the knee, ankle, and shoulder. A few exercises to provide stiffness of the lower back are presented later in this chapter.
Muscles contributing to lumbar stiffness
Muscles such as the transversus abdominis, obliquus internus, diaphragm, iliocostalis, multifidus, and quadratus lumborum have been suggested to be active in protecting and stabilizing the lumbar spine. Of the local muscles, the transversus abdominis and the lumbar multifidus are the most discussed and studied muscles to especially contribute to lumbar stiffness. However, since the transversus abdominis muscle works closely with, and sometimes fuses with, the obliquus internus, the obliquus internus may also be considered an important contributor to the stiffness of the lumbar spine. The transversus abdominis is the abdominal muscle most closely associated with control of intraabdominal pressure and it also influences stiffness and intersegmental motion of the lumbar spine through its connection to the thoracolumbar fascia. Furthermore, this muscle preactivates during a movement of the upper or lower extremity, even before the primary movers of the actual extremity. This activation is delayed in patients with low back pain. The multifidus muscles are best developed in the lumbar region of the spine and their contribution to lumbar stiffness has been shown in a variety of studies. These muscles are impaired in patients with low back pain and recovery of the multifidus muscles does not appear to be automatic after resolution of an acute, first-episode of low back pain.
Prevention of nonspecific low back pain
Injury involving the low back is not uncommon among gymnasts and low back pain is a common complaint. Specific segmental exercises of the lumbar muscles have shown promising results regarding treatment and prevention of low back pain in young teamgym gymnasts (Harringe et al., 2007). The idea is to add specific, low-intensity exercises to the lower back, as a complement to the ordinary strength and preparation training for gymnasts. The exercises should be implemented in the regular training, for example, in the warm-up, and be continuously performed. This type of training has also been used with success in the treatment of more severe injuries such as disc herniations and spondylolysis (O’Sullivan et al., 1997). However, it is important to remember that the exercises do not replace ordinary trunk muscle training. A study on collegiate gymnasts performing a 15-minutes general trunk muscle training program, twice a week, 10 weeks preseason, also appeared to reduce episodes of low back pain (Durall et al., 2009). As long as there is no fatigue or injury the core muscles work properly and co-activate without specific exercises. However, once there is disturbed activity such as fatigue or injury the deep stabilizing muscles do not work properly. To ensure well-functioning core muscles, the specific exercises should be introduced as a complement to ordinary trunk muscle training.
Specific exercises for lumbar stiffness
In the early 1990s, Richardson and Jull (1995) presented specific muscle exercises to control the lumbar spine. The specific exercises were suggested to reactivate the local muscles of the lumbar spine and to control pain in patients with low back pain. The base for this training is the draw-in action, also called abdominal hollowing. It is an isometric muscle contraction to not only activate the transversus abdominis and/or obliquus internus but also enhance co-activation with the lumbar multifidus muscles. The abdominal hollowing is performed by gently drawing in the abdominal wall, especially of the lower abdominal area. It is an isometric contraction and the time length for which the exercise is held, as well as to maintain a normal rate of breathing, is important. A pressure bio-feedback unit (Chattanooga group, Inc., USA) (Figure 14.2) may be used to control for correct muscle contraction.
Figure 14.2 A pressure bio-feedback unit. The unit is inflated to 70 mmHg pressure and placed under the lower abdomen while the subject is lying in prone position. When the correct contraction is performed, pressure decreases by approximately 6–8 mmHg.
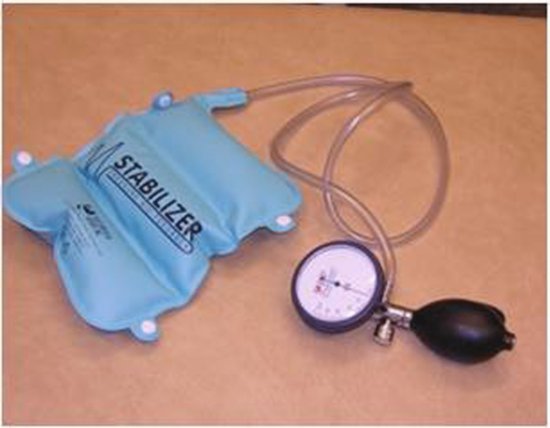
The device is helpful, in particular during the learning phase, for guidance of performing the muscle contraction correctly. The specific training is commenced in the four point kneeling and prone positions, of which the four point kneeling position may be the easiest to start with (Figure 14.3). In this position the rectus abdominis muscle is difficult to activate and thus helpful since the aim of the training is to activate the deeper part of the abdominal wall. Once the gymnast knows how to perform the exercise, the positions should become more sport-specific. The gymnast may, for example, perform the abdominal hollowing in a static position such as a handstand or in a dynamic situation walking on the hands or in a tumble or a vault (see Weeks 5–8 in Section “Eight-weeks introduction program”). However, it is important to keep one or two of the basic exercises to ensure correct performance and to ensure a reactivation of potentially fatigued muscles. The bio-pressure feedback unit is fun to use and, when used correctly, provides accurate feedback.
Figure 14.3 Abdominal hollowing in a prone and a four point kneeling position. (Source: Harringe et al. (2007) with kind permission from Springer Science and Business Media.)
Eight-weeks introduction program
Hereunder an introduction program to the specific muscle control exercises is presented (Harringe et al., 2007). The idea is to introduce an exercise to reactivate fatigued or injured deep stabilizing muscles of the lower back. It should be implemented during ordinary training. Once the gymnasts master the abdominal hollowing it may be an exercise to use in the warm-up, just to make sure that the muscles work properly, or in different training modalities for core stability. There are several books on core stability or core training and these may give ideas on how to progress with the training. However, the key to success is to keep it simple in the learning phase to be sure to target the deep muscles. Remember that these exercises complement heavy load training and it is important to ensure correct technique in the exercises.
Weeks 1–2: Introduce the abdominal hollowing in prone and four-point kneeling positions (Figure 14.3). Use the pressure bio-feedback unit (Figure 14.2) to control for correct execution in prone position. Each exercise should be repeated 10 × 10 seconds and included in the warm-up.
Weeks 3–4: Keep the basic exercise in the four-point kneeling position. Add diagonally elevation of the arm and leg in the prone position. Repeat each exercise 10 × 10 seconds. Also add abdominal hollowing in an upright position on a balance board. Position the body on both feet, with slightly flexed knees while moving the arms up and down in front of the body. The exercise is easy to perform, although it increases the demands on the deep stabilizers of the lumbar spine. The exercise should be performed for 5 minutes at each training session. To increase the difficulty the gymnast may add some weight, for example, light dumbbells in the hands, while moving the arms up and down. However, it is important to keep the control of the abdominal hollowing during the exercise.
Weeks 5–8: Continue with the exercises from previous weeks. Add sports-specific positions with the instruction to keep emphasis on the abdominal hollowing. In the study on teamgym gymnasts by Harringe et al. (2007), 12 basic trampette skills were added. Unstable surfaces such as balance boards, trampolines, and trampettes have shown to activate stabilizing muscles of the lumbar spine and thus improve core stability. The sports specificity of the exercises should be chosen to fit the different disciplines.
Prevention of lower extremity injuries
The lower extremity is the most commonly injured body region in Artistic Gymnastics. Injuries involving the knee and ankle, in particular, occur frequently in Artistic Gymnastics (see Chapter 10). There is little gymnastics-based evidence on how to prevent these injuries, although some studies, in other sports, suggest that general strength training, neuromuscular control exercises, and plyometric strength training may reduce injuries to the lower extremity (Schiff et al., 2010). Unpublished data on recreational gymnasts suggest that plyometric training may improve the gymnasts’ performance and reduce the frequency of knee injuries and a limited study on young artistic female gymnasts showed reduced pain with neuromuscular control exercises (Marini et al., 2008).
In studies on soccer and European team handball different control and balance exercises combined with plyometric training have reduced the incidence of anterior cruciate ligament injuries (Schiff et al., 2010). Exercises including cutting and landing have been used and may also be useful in gymnastics since many injuries occur due to poor landing technique, and specific focus on landing has been proposed in the prevention of gymnastics injuries. Plyometric strength training engages the muscle-tendon stretch-shortening cycle and studies have shown rapid effects on strength gain with this type of technique. A newly published study set up in a biomechanics laboratory concluded that only one training session (six sets of three repetitions) using a countermovement jump may improve performance through neural modulation (Hirayama et al., 2012). This could possibly mean that this technique may help the gymnasts to regain neural control after intensive gymnastics training. However, the plyometric training is intensive and should not be performed when the gymnast is tired. Most studies implement the prevention exercises in the warm-up and the most successful prevention programs have been carried out during the entire season, linked to education of coaches and athletes. Further studies are needed in order to establish its role in gymnastics injury prevention.
Prevention of upper extremity injuries
Injuries to the upper extremity (e.g., shoulder or wrist) are more common in male gymnasts compared to female counterparts (in whom ankle and lower back injuries predominate) possibly due to the different types of apparatus used in men’s gymnastics. However, wrist pain, as well as more severe wrist injury, is common in the young growing gymnast. Most scientific work in this field consists of case reports and some studies suggest possible, though not tested, preventive strategies (DiFiori et al., 2006). Strength training and stabilizing exercises as well as taping or bandaging are frequently used in ordinary training. Biomechanical and clinical studies indicate that protective wrist bracing may prevent acute wrist injury; however, this preventive measure has not been tested in a controlled trial on gymnasts. Another approach would be to reduce the impact by alternating between different skills such as swinging and support-type movements during practice. An optimal gymnastics technique and recovery can most probably minimize the high impact on the body structures.
Muscle and joint symmetry
A decreased joint or muscle range of motion may result in bad timing and asymmetric force transformation through the body. Using the take-off going into a tumble or vault as an example, the forces are transformed from the ankle through the body into the gymnastics skill. The timing has to be exact in order to perform the perfect skill. If there is an asymmetry in muscle or joint range of motion the forces may be unevenly transformed and possibly result in poor technique and increased risk of injury. This is of course even more important in advanced skills since the forces are greater and consequently the impact on the gymnast higher. A slight mistake may be devastating. Equal attention to the right and left side is necessary and may prevent injuries.
Mental preparation
It is not necessarily the most difficult skills that cause acute injury. It has been shown that gymnasts are often injured in skills they know well. Since gymnastics is a very demanding sport and focus and control are qualities needed, mental preparation should be included in the prevention of injury. It would seem important to put emphasis on quality of workouts rather than repetitiveness at all times. Imagery techniques that cause no physical impact may allow a gymnast to train more hours without increased injury risk. However, the role of mental practice in reducing injuries has not been investigated in gymnastics.
An interesting but underresearched area of injury risk in gymnastics is the role played by psychosocial factors. A relation between extent of negative life stress and the frequency and severity of injury has been reported in several studies. It would seem important that gymnasts be encouraged to share with their coach, medical personnel, and parents any concerns they might have, including difficulty of skills practiced or pain experienced. “No pain—no gain” is inappropriate in gymnastics.
Extrinsic strategies
Safety equipment and gymnastics apparatus
Safety equipment such as foam pits, trampolines, bungee straps, and spotting belts are frequently used in daily practice sessions. This equipment is helpful not only in reaching new levels of performance but also in reducing the impact and risks for injuries to occur. The apparatus and landing mats have changed over time due to the continuous development of the sport, not only with respect to level of performance but also due to the protection of the gymnasts. During the last 10 years, new landing material to reduce the ground reaction forces has been introduced. These mats seem to put more strain on the forefoot, but less total ground reaction force. The construction and model/form of the vaulting apparatus (the new Pegasus) to lower the incidence of head and neck injuries, and the coverage around the trampolines and springboards are also examples on what has been done to prevent and reduce the incidence of injuries in gymnastics. However, the effectiveness of these preventive measures has not been investigated.
Health support system
Regular medical check-ups are important and necessary in prevention of injury. However, medical monitoring of gymnasts is rare in gymnastics settings below the college level. We recommend a preparticipation physical examination (PPE) for each gymnast prior to entry in competitive gymnastics, before any change in competitive level, and before returning to practice following injury. The medical history and physical examination can identify underlying conditions that require special attention or that predispose the gymnast to injury unless appropriate preventive measures are followed.
Gymnasts are generally young and growth should be monitored closely, especially since the injury risk may increase during periods of rapid growth. Research has shown that physeal strength is decreased during pubescence. Furthermore, bone mineralization may lag behind bone linear growth during the growth spurt, leading to an increased risk for injury. It is important and may be injury preventive to individualize training and skill development to accommodate possible size, physique, strength, performance, and maturity differences among chronological age peers. Thorough medical check-ups should be carried out to keep track of growth and maturation as well as nutrition, recovery, and overload. If risk behavior or pain can be captured early in time, injuries may be avoided or at least the severity of the injuries reduced.
We also recommend that gymnastics clubs include within their cost structure sufficient funds to hire an athletic trainer, physical therapist and/ or a physician with interest/expertise in sports injuries, at least on a part-time basis. This health professional should be available to provide immediate care of injuries and to supervise rehabilitation as well as to oversee special rehabilitation programs for injured or injury-prone gymnasts prior to returning to practice and competition. Early recognition of injury is important, and is improved by the presence of competent medical personnel. If the availability of a trainer or therapist is limited, their time is perhaps best focused on advanced-level gymnasts who appear at greatest risk of injury.
Gymnastics is a very demanding sport as well as an aesthetic sport. This may lead to body fixation and an increased risk for developing sports anorexia. Low levels of nutrition may lead to decreased performance and injury. A recent study reported low levels of vitamin D in elite female gymnasts (Lovell, 2008). Other studies have shown low total energy intake as well as low levels of micronutrients such as iron, zinc, and calcium (Caine et al., 2001).
If possible, a multidisciplinary team including coaches, medicine support staff, nutritionists, and psychologists should be working together regarding the strategies for prevention of injury.
Training diary and periodic planning
A training diary may be useful in detecting and preventing the gymnast from injury. A diary should be easy to fill out and may contain preprinted questions. It should include training parameters such as skill level, training volume, training intensity, and training quality. The diary should also include other important factors for optimal performance such as how the gymnast feels today—alert or tired, and other outside gymnastics events that may interfere with gymnastics and rest and sleeping quality. Furthermore, a diary is helpful in planning the practice and in the transition from skill training to routine training. This transition takes time and should be well planned.
Full routines put another type of strain and demand on the gymnast. An emphasis on quality of workouts rather than repetition may be injury preventive. It is important to slowly increase the intensity and carry over from regular preparation and practice to full routine performance and competition. A perfect technique is necessary to decrease the risk for injury and therefore the gymnast has to be well prepared and only perform skills and routines he or she feels secure with during competition.
Education
Education is important and may provide coaches, gymnasts, and parents with knowledge important for the right decisions to be made regarding injury prevention. Through education the coaches should keep themselves updated with respect to changes in gymnastics including equipment and apparatus, skill techniques and levels of difficulty. In addition, education should include knowledge about growth and maturation of children and adolescents as well as an understanding that an injury, especially if insufficiently rehabilitated, may predispose the gymnast to another injury or recurrence of the same injury. A coach has to have adequate and demonstrated gymnastics competence for the level of gymnastics he or she is teaching. We recommend that in order to be hired as a gymnastics coach he or she should meet a minimum level of qualification as determined by the national gymnastics federation. With the USA Women’s Artistic Gymnastics program, for example, one may achieve four progressive certification options: (1) Instructor, (2) Jr. Olympic Development Coach, (3) Jr. Olympic Team Coach, and (4) National Coach. Each certification offers a unique set of courses to equip coaches with the knowledge required to achieve excellence and better ensure the safety of gymnasts.
The first line of protection from injury belongs with the gymnast. A well-educated and thoroughly trained gymnast may detect and avoid potentially injurious situations. Furthermore, the gymnast has to be educated from an early age to distinguish between different types of pain and to listen to the signals from his or her body. Pain may signal possible or actual injury, or the achievement of optimum workload to produce a physical conditioning effect. Studies have shown that young gymnasts are capable of distinguishing between soreness from exertion and acute pain owing to injury. This is important knowledge, and may help the gymnast and those surrounding him or her to make better decisions about pain management and continued practice.
Further research
There is no doubt that gymnastics participation brings with it a wealth of personal and health-related benefits. Physical activity reduces the risk of premature mortality in general, and of coronary heart disease, hypertension, colon cancer, obesity, and diabetes mellitus in particular. However, gymnastics participation may also give rise to injury, which may undermine the many benefits of being physically active and contribute to long-term disability. Establishing sound epidemiologic research to determine the rate and severity of gymnastics-related injury and then using these data as basis for systematically identifying risk factors and developing effective prevention interventions is imperative.
Gymnastics lacks good-quality descriptive data, the fundamental building blocks of epidemiology, and which provides a basis for conducting meaningful analytical studies. This is reflected in the generally sparse listing of intrinsic and extrinsic risk factors and the extreme paucity of epidemiologic studies on preventive measures (see Chapter 10). Furthermore, most of the epidemiological research on injury in gymnastics was published prior to 2000, a major concern given the ever-changing nature of skills practiced and performed in this sport. This finding is especially disturbing given the young age of many gymnastics athletes and the relatively high incidence and severity of gymnastics injury reported in the literature.
There is a pressing need for studies designed to test risk factors and to identify and determine the effect of injury-prevention measures on reducing the rate of injury among gymnasts. Injury-prevention measures of particular interest include neuromuscular training programs, preseason conditioning, programs to enhance landing and skill mechanics, and use of taping and bracing to prevent ankle and wrist injuries. It is imperative that gymnastics organizations, including artistic, rhythmic, and trampoline, sponsor ongoing injury surveillance systems to provide an accurate picture of the incidence and severity of gymnastics-related injury and to serve as a basis for identifying and testing risk factors and preventive measures. Descriptive epidemiological studies inform us that injuries and conditions such as ankle sprains, heel pain, wrist pain, and low back pain occur frequently in gymnastics and require special attention. Increased frequency of injury following periods of competitive routine preparation, as well as per unit time during competition, also signal increased attention.
Summary
Prevention of injuries is highly important and has to be central for the team surrounding a gymnast. Few studies have investigated prevention programs and therefore little epidemiological evidence is available on how to actually prevent injuries in gymnastics. However, this chapter provides the reader with a summary of what we know today and can understand from previous epidemiology studies and health care professionals’ experience. The basics of prevention must be to understand the sport, implement correct technique, and be sure to obtain adequate and complete recovery. Further research, including injury surveillance systems, is definitely needed to prevent gymnastics injuries and establish guidelines for gymnasts and coaches in the future.
References
Caine, D., Lewis, R., O’Connor, P., Howe, W., and Bass S. (2001) Does gymnastics training inhibit growth of females? Clinical Journal of Sports Medicine, 11, 260–270.
DiFiori, J., Caine, D., and Malina, R. (2006). Wrist pain, distal radial growth plate injury, and ulnar variance in the young gymnast. American Journal of Sports Medicine, 34, 840–849.
Durall, C.J., Udermann, B.E., Johansen, D.R., Gibson, B., Reineke, D.M., and Reuteman, P. (2009) The effects of preseason trunk muscle training on low back pain occurrence in women collegiate gymnasts. Journal of Strength and Conditioning Research, 23, 86–92.
Harringe, M.L., Nordgren, J.S., Arvidsson, I., and Werner, S. (2007) Low back pain in young female gymnasts and the effect of specific segmental muscle control exercises of the lumbar spine: a prospective controlled intervention study. Knee Surgery, Sports Traumatology, Athroscopy, 15, 1264–1271.
Hirayama, K., Yanai, T., Kanehisa, H., Fukunaga, T., and Kawakami, Y. (2012) Neural modulation of muscle-tendon control strategy after a single practice session. Medicine and Science in Sports and Exercise, doi: 10.1249/MSS.0b013e3182535da5.
Lovell, G. (2008) Vitamin D status of females in an elite gymnastics program. Cinical Journal of Medicine, 18, 159–161.
Meeuwisse, W. and Bahr, R. (2009) A systematic approach to sports injury prevention, Chapter 2. In: R. Bahr and L. Engebretsen (eds), Handbook of Sports Medicine and Science. Sports Injury Prevention, An IOC Medical Commission Publication. Wiley-Blackwell Publishers, West Sussex.
Marini, M., Sgambati, E., Barni, E., Piazza, M., and Monaci, M. (2008) Pain syndromes in competitive elite female artistic gymnasts. Role of specific preventive-compensative activity. International Journal of Anatomy and Embryology, 113, 1–8.
O’Sullivan, P.B., Twomey, L.T., and Allison, G.T. (1997) Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine, 22, 2959–2967.
Richardson, C.A. and Jull, G.A. (1995) Motor control – pain control. What exercises would you prescribe?. Manual Therapy, 1, 2–10.
Schiff, M., Caine, D., and O’Halleron, R. (2010) Injury prevention in sports. American Journal of Lifestyle Medicine, 4, 42–64.
Van Mechelen, W., Hlobil, H., and Kemper, C.G. (1992) Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Medicine, 14, 82–99.
Recommended reading
Bahr, R. and Engebretsen L. (eds) (2009) Handbook of Sports Medicine and Science. Sports Injury Prevention. An IOC Medical Commission Publication. Wiley-Blackwell Publishers, West Sussex.
Bahr, R. (2003) Preventing sports injuries. In: R. Bahr and S. Maehlum (eds), Clinical Guide to Sports Injuries, pp. 41–53. Human Kinetics, Champaign, IL.
Hootman, J.M., Dick, R., and Agel, J. (2007) Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention. Journal of Athletic Training, 42 (2), 311–319.
Jemmett, R. (2003) Spinal Stabilization, The New Science of Back Pain. 2nd edn. Novant Health Publishing, Halifax, NS.
Kolt, G. and Caine, D. (2010) Gymnastics. In: D. Caine, P. Harmer and M. Schiff (eds), Epidemiology of Injury in Olympic Sports. Encyclopaedia of Sports Medicine, vol. XVI, pp. 144–160. Wiley Blackwell Publishers (UK) and the IOC Medical Commission.
Schiff, M. and O’Halleron, R. (2010) Injury prevention in sports. In: D. Caine, P. Harmer, and M. Schiff (eds), Epidemiology of Injury in Olympic Sports. Encyclopaedia of Sports Medicine, vol. XVI, pp. 491–499. Wiley Blackwell Publishers (UK) and the IOC Medical Commission.
USA Gymnastics (2009) Safety Course Handbook: Gymnastics Risk Management. USA Gymnastics, Inc. Indianapolis, IN.
Weaver, J., Moore, C., and Howe, W. (1996) Injury prevention. In: D Caine, C. Caine, and K. Lindner (eds), Epidemiology of Sports Injuries, pp. 439–447. Human Kinetics Publishers, Champaign, IL.
< div class='tao-gold-member'>




