3.1 Gastrointestinal disease
Chapter 3.1a The physiology of the gastrointestinal system
At the end of this chapter you will be able to:
Estimated time for chapter: Part I, 60 minutes; Part II, 60 minutes.
PART I – From our food to the stomach

The nutrients in our diet
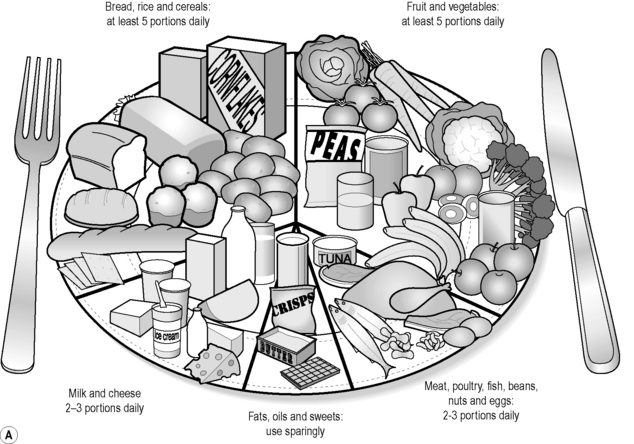
A healthy diet will consist largely of starchy foods such as bread, rice, pasta and cereals, and fruit and vegetables. Current UK guidelines for the public are that about 60% of the energy value of food (calories) should come from starchy foods and that additional energy should come from at least five portions of fruit or vegetables a day. In addition, there should be some food containing protein, either from the meat/eggs/pulses food group or from the milk/cheese food group. Foods containing fats and sugars should be kept to a minimum. The UK Food Standards Agency ‘eat well plate’ summarises this advice in pictorial form as shown in Figure 3.1a-I.
Carbohydrates
Starchy foods and fruit and vegetables together provide the carbohydrates that the body needs. Carbohydrates contain the elements carbon, hydrogen and oxygen. These are the foods that, once broken down, provide the basic fuel for the energy-producing process of internal respiration (see Chapter 1.1b). Internal respiration takes place in the mitochondria of all living cells, where simple sugars react with oxygen to produce cellular energy. Carbon dioxide and water are the waste products. The energy produced is stored partly in the form of the ‘charged’ molecule adenosine triphosphate (ATP), and is partly released as heat.
Proteins
Proteins are complex chain-like structures that are made up of simple molecules called ‘amino acids’. All amino acids contain the element nitrogen as well as carbon, hydrogen and oxygen. Some also contain trace minerals such as zinc, iron and copper. There are about 20 different amino acids, which can be combined in potentially infinite permutations to form protein chains. Proteins are made in animal and plant cells at the ribosomes as a result of decoding instructions held on the cellular DNA (see Chapter 1.1b). The ribosome is the site at which amino acids are linked together to form a unique and characteristic protein chain, after which the particular makeup of the protein chain encourages the structure to fold in a characteristic way. This means that proteins are large molecules that have a unique shape. The shape and form of a particular protein might give it special structural properties (e.g. the collagen in skin and hair) or make it soluble in water (e.g. the albumen found in blood and in egg white). In other proteins the shape is essential for communication, and this is the basis of how cell-membrane proteins ‘recognise’ the external stimulants, such as hormones, that bring about internal change in the cell itself. Antibody–antigen recognition also depends on the antibody having a unique shape that ‘fits’ the shape of the antigen.
Vitamins
Vitamins are more complex compounds than minerals, and are also essential for bodily processes. They are essential dietary components because either they cannot be made by the body at all or they cannot be made in sufficient quantities to sustain health. Vitamins are now broadly grouped into the four fat-soluble vitamins A, D, E and K, and the nine water-soluble vitamins B1–B8 and C. The lettering system approximately relates to the order in which the vitamins were discovered (beginning with vitamin A in 1909). Those substances initially called F–J were either reclassified as B vitamins or were subsequently deemed not to qualify as vitamins at all. The B vitamins are now recognised to be linked because they are all vital in the production of energy from nutrients by the mitochondria. The food sources and the functions of the 13 vitamins are summarised in Table 3.1a-I.
Table 3.1a-I The 13 vitamins, their main food sources and their functions in the body
| Vitamin | Food sources | Use in the body |
|---|---|---|
| A (retinol) | Green vegetables, milk, liver | Pigments in eye and health of skin |
| D (calciferol) | Milk, eggs, cod liver oil; ultraviolet light | Calcium absorption and bone formation |
| E (tocopherol) | Margarine, seeds, green leafy vegetables | Antioxidant: protects fatty acids and cell membranes from damaging oxidation |
| K (phylloquinone) | Green leafy vegetables | Formation of certain clotting factors |
| B1 (thiamine) | Meats (pork), grains, legumes | Carbohydrate metabolism; also nerve and heart function |
| B2 (riboflavin) | Milk, liver, eggs, grains, legumes | Energy metabolism |
| B3 (niacin or nicotinic acid) | Liver, lean meats, grains, legumes | Energy metabolism |
| B5 (pantothenic acid) | Milk, liver, eggs, grains, legumes | Energy metabolism |
| B6 (pyridoxine) | Wholegrain cereals, vegetables, meats | Amino acid metabolism |
| B7 (biotin) | Meats, vegetables, legumes | Fat synthesis and amino acid metabolism |
| B9 (folic acid) | Wholewheat foods, green vegetables, legumes | Nucleic acid metabolism |
| B12 (cobalamin) | Red meats, eggs, dairy products | Nucleic acid production |
| C (ascorbic acid) | Citrus fruits, green leafy vegetables, tomatoes | Collagen formation in teeth, bone, and connective tissue of blood vessels; may help in resisting infection |
Water
 Information Box 3.1a-I
Information Box 3.1a-Iper day. Any water excess to requirements is passed out of the body in the form of dilute urine. If insufficient water is drunk, the kidneys make dark concentrated urine from the fluid in the plasma, and the water required for excretion of wastes is drawn from the tissues, which then become dehydrated. A significant state of dehydration will be reflected in a loss of body weight of more than 2–3%. Because the sensitive tissues of the body are not able to withstand the state of dehydration for more than a few days, water is essential for life. Loss of more than 10% of the body weight through dehydration is usually not compatible with life  (see Q3.1a-2-Q3.1a-6).
(see Q3.1a-2-Q3.1a-6).
The structure of the digestive tract
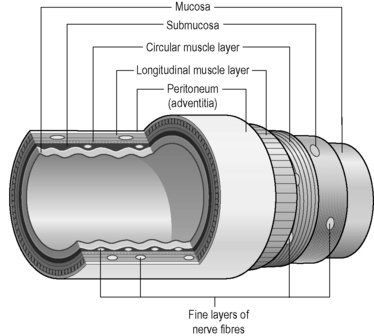
The tube of the digestive tract has a basic structure that can be found in slightly different forms along its length. The tube has four distinct layers (Figure 3.1a-II):
• The adventitia is the outer layer of the digestive tract. Below the diaphragm, the adventitia forms the peritoneum which is a serous membrane (i.e. it secretes watery fluid). This protects and lubricates the digestive tract so that it can move easily within the abdominal cavity.
• The muscle layer consists of two layers of smooth muscle. The longitudinal and circular fibres contract in coordinated waves to propel the contents of the food down the length of the tract. This motion is called ‘peristalsis’.
• The submucous layer is a layer of connective tissue that contains blood vessels, collections of lymph nodes, lymphatic vessels and networks (plexuses) of nerves.
• The mucosa consists of a mucous (epithelial) membrane (see Chapter 1.1d), with its combined functions of protection, secretion and absorption, and two supportive layers beneath this. The mucous membrane secretes mucus for further protection and lubrication. Other specialised cells in the mucous epithelium are sensitive to changes in the contents of the digestive tract. These secrete hormones into the blood stream within the submucous layer.
The mouth is the only section of the digestive tract that does not have this general structure.
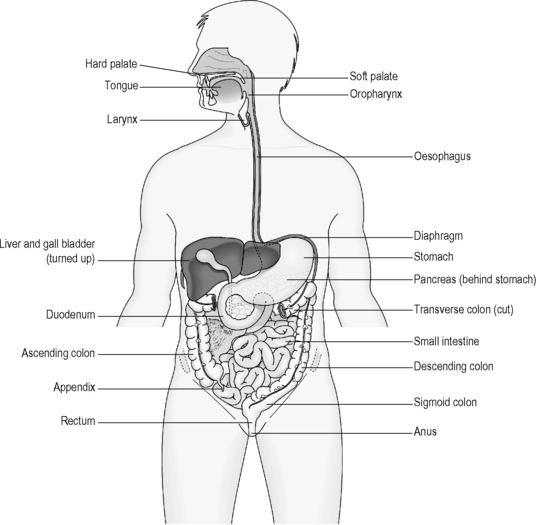
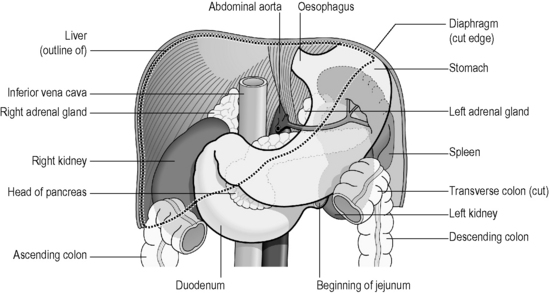
The salivary glands open via tubes (ducts) into the mouth, the pancreas, liver and gallbladder all open via ducts into the duodenum, and the appendix opens directly into the beginning of the colon. Figure 3.1a-III illustrates the position of the organs associated with the digestive tract, and how, with the exception of the mouth and the oesophagus, the main part of the digestive tract is situated below the diaphragm.
The mouth
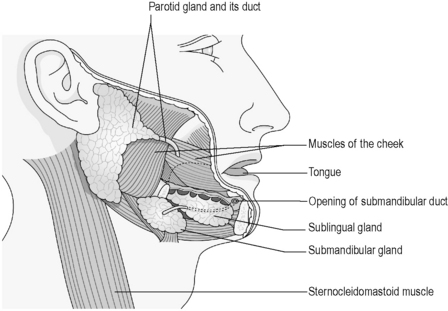
Saliva is produced by six exocrine salivary glands that open into the mouth. The size and extent of these important glands is illustrated in Figure 3.1a-IV.

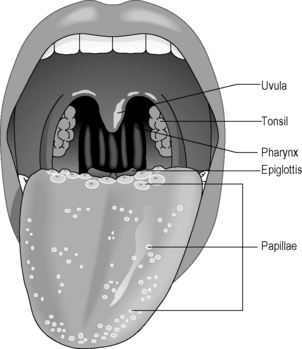
The tongue is a muscular structure adapted for two distinct functions: eating (taste, chewing and swallowing) and speech. It is covered with little bumps called ‘papillae’, which are sensitive to the four main tastes: salt, sweet, sour and bitter. The subtleties of taste are also dependent on a healthy sense of smell, as anyone who has a heavy cold will recognise. Figure 3.1a-V illustrates the position of the different sorts of papillae.
The stomach
The stomach is a stretchy expansion of the tube of the digestive tract, but still retains the four layers. Figure 3.1a-VI illustrates that the stomach is bounded by the cardiac sphincter above and the pyloric sphincter below. These muscle rings keep food contents within the stomach for up to 6 hours to enable the beginning of a thorough digestion process. The stomach muscles enable the muscle to churn the food contents stored within it to aid digestion.

PART II – From the duodenum to the outside world
The duodenum (the first part of the small intestine)
 Information Box 3.1a-II
Information Box 3.1a-IIThe pancreas
The pancreas is a gland with two distinct roles, one is endocrine and the other is exocrine. (For a reminder of the difference between these two categories of epithelial structure, see Chapter 1.1d.)
 Information Box 3.1a-III
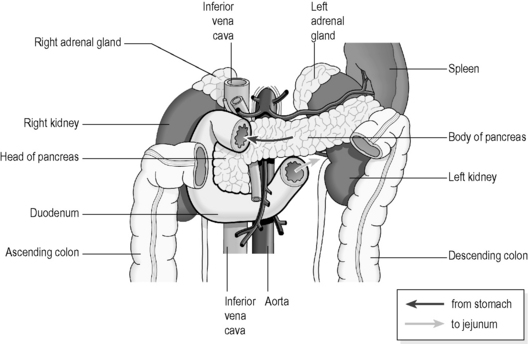
Information Box 3.1a-IIIFigure 3.1a-VII illustrates how the C-shaped loop of the duodenum hugs the pancreas. The spleen, kidneys, liver and transverse colon are all situated at this level of the abdomen
The gallbladder
 Information Box 3.1a-IV The anatomy of the organs associated with the duodenum: comments from a Chinese medicine perspective
Information Box 3.1a-IV The anatomy of the organs associated with the duodenum: comments from a Chinese medicine perspective
Note from Figure 3.1a-VII that the spleen lies at the same level as the pancreas. It is possible that the ancient Chinese assumed that the pancreas and spleen were one anatomical organ, as the pancreas is never directly referred to in the classics of Chinese medicine. Anatomically the two organs are very closely related and share a common blood supply. This may explain why digestive functions were attributed to the Spleen. However, the spleen is conventionally considered to have its main role in the lymphatic system, with absolutely no part to play in the digestion of food. It is also interesting to see that the kidneys are also at this level in the body, and very close by are the liver, gallbladder, and loops of the large and small intestines.
include a deeply hued chemical called ‘stercobilin’ (derived from the breakdown of haemoglobin), which gives the faeces their characteristic brown colour.
The small intestine
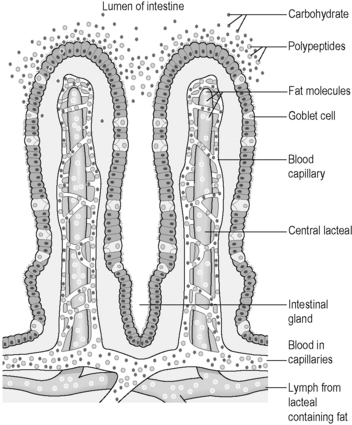
The small intestine is about 5 metres long, and its lining is thrown into folds. Microscopic peaks of mucosa project from these folds, and appear, when greatly magnified, like a vast mountain range. These peaks are called ‘villi’. Furthermore, each cell of the mucosa has tiny projections called ‘microvilli’. This unique structure greatly increases the area of the mucosa that is in contact with the fluid contents of the digestive tract, an adaptation that maximises absorption. Figure 3.1a-VIII illustrates the microscopic structure of a villus, including the tiny microvilli on each cell, and also the way the blood and lymph supply of the digestive-tract lining project into the centre of the villus.

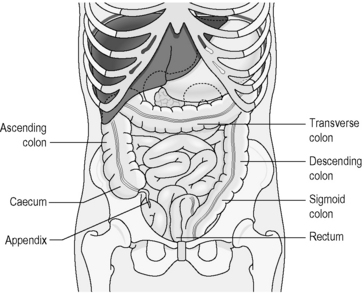
The large intestine
The large intestine, or colon, receives the residue of digestion from the small intestine. The first few centimetres of the colon are called the ‘caecum’, which literally means ‘blind ending’. This is because it is above the caecum that the end of the small intestine opens into the colon, with the result that the caecum is like a cul-de-sac opening out from the passage. At the end of this cul-de-sac is the narrow tube of the appendix. The parts of the large intestine are illustrated in Figure 3.1a-IX. Note how the horizontal stretch of the transverse colon overlies the duodenum and pancreas at the level of the T12 thoracic vertebra.
The large intestine is the home for most of the ‘healthy’ bacteria and yeasts which were first described in Chapter 2.4b. The food residue that enters the large intestine is digested further by these ‘healthy’ organisms. The by-product of this digestion is gas, which is eventually passed out of the anus. Some necessary vitamins are made as by-products of this process, which can then be absorbed into the bloodstream.

The liver
Other roles of the liver include:
• The use of amino acids to make the proteins carried within the plasma (including the clotting factors).
• The removal of worn-out red blood cells. The spleen has the main responsibility for this function (see Chapter 3.4a), but is assisted in this task by the liver. Phagocytic white blood cells in the spleen and the liver digest the old red blood cells and then release many of the by-products of digestion into the blood for reuse by the body. The waste product of this process is bilirubin, the green-yellow coloured substance that is excreted into the bile.
• To be a source of heat. The liver is such an active organ that it is one of the most important sources of heat for the body.
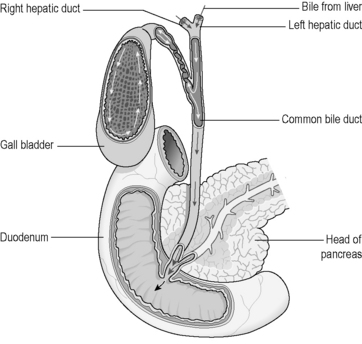
The last role to be described here is that of the secretion of bile. In addition to the diverse functions already listed, all the liver cells are able to produce bile and secrete it into tiny tubules in the liver. From here, the bile drains into a duct that leaves the liver and enters the duodenum. The gallbladder also opens into this duct, so that the bile collects here rather than passing directly into the duodenum (Figure 3.1a-X).
 Information Box 3.1a-V The liver: comments from a Chinese medicine perspective
Information Box 3.1a-V The liver: comments from a Chinese medicine perspective
For more detail on the correspondences between the functions of the liver and gallbladder as described in conventional medicine and the Liver and Gallbladder Organs in Chinese medicine, see Appendix I.
Figure 3.1a-X helps to illustrate how the gallbladder can be surgically removed without disturbing the free flow of bile from the liver. The function of the gallbladder is simply to delay the entry of bile into the duodenum until the best time for digestion of fats. Removal of the gallbladder results in a constant trickle of bile into the duodenum. This is not ideal for perfect digestion of fats, but is not conventionally considered to be a problem for overnourished western people.
The metabolism
Metabolism can be broadly considered in two categories:
• Anabolism includes all those reactions that lead to the building up of new substances for cellular growth or function (this might be described as a Yin process in Chinese medicine language).
• Catabolism includes all those reactions that lead to the breakdown of the complex structures of the cell, and often leads to the release of energy (this might be described as a Yang process in Chinese medicine language).
 Information Box 3.1a-VI
Information Box 3.1a-VI Self-test 3.1a The physiology of the gastrointestinal system
Self-test 3.1a The physiology of the gastrointestinal system
1. What are the six basic nutrients to be found in our diet?
2. What are the essential basic nutrients that are transported, after digestion, from the digestive tract to the cells?
3. What components in the diet are digested in the stretch of digestive tract from the mouth to the stomach?
4. How do pancreatic juice and bile contribute to the process of digestion of the food?
5. How is the small intestine adapted to its function of the absorption of food?
6. What nutrients are absorbed from the colon?
7. List six main functions of the liver.
Answers
1. Carbohydrates, proteins, fats, vitamins, mineral salts and water.
2. The essential nutrients that are transported to the cells after digestion are:
3. Carbohydrates are broken down to saccharides by the enzymes in saliva, and proteins are broken down to amino acids in the stomach. The chewing of food and the churning action of the stomach turn the solid diet into a fluid ready for further digestion in the small intestine.
4. Pancreatic juice contains enzymes, which further break down carbohydrates into saccharides and proteins into amino acids. These enzymes also digest some fats (not including cholesterol, which is absorbed unchanged) into fatty acids, and glycerol. Bile salts in the bile aid the digestion of fatty acids.
5. The small intestine is adapted to maximise absorption by being very long and in the structure of its mucosa, which has folds, villi and microvilli to increase the surface area further. The blood and lymphatic supply of the small intestine is very rich and is arranged so that a blood vessel and a lymphatic vessel project into each of the thousands of villi on the mucosa.
6. The colon absorbs about two-thirds of the water that enters it, and also some essential vitamins that are the by-products of digestion by colonic microorganisms.
7. The functions of the liver include:
Chapter 3.1b The investigation of the gastrointestinal system
Investigation of the gastrointestinal system
The investigations that are most likely to reveal information about the digestive tract include:
• a thorough physical examination
• tests to ‘visualise’ the inside of the gastrointestinal tract and the accessory organs, including endoscopy, X-ray studies with barium contrast, and ultrasound and computed tomography (CT) scans
• tests to remove samples of tissue for examination (biopsy).
These tests are considered briefly below in turn.
Physical examination of the gastrointestinal system
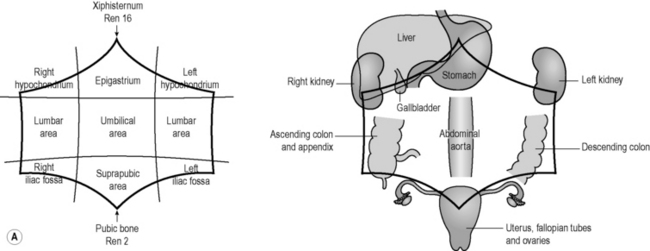
The physical examination of the gastrointestinal involves the stages listed in Table 3.1b-I. For the purposes of physical examination of a supine patient, the accessible region of abdomen is considered to occupy the approximately hexagonal region that is bounded by the ribs above and the inguinal ligaments and pubic bone below.
Table 3.1b-I The stages of physical examination of the gastrointestinal system
As Figure 3.1b-I illustrates, many important organs are situated underneath the nine named regions of the abdomen. A lump felt in the suprapubic area, for example, might suggest a problem of the bladder or the uterus, whereas pain in the left iliac fossa would suggest a problem of the colon or left ureter. The names for these nine regions of the abdomen are frequently used in medical texts for the description of abdominal conditions, so it is useful to be familiar with them.
Blood tests
The two most common tests are:
• Full blood count (see Chapter 2.4d). This is the test used to exclude the anaemia that can result from long-term bleeding in conditions such as a chronic stomach ulcer.
• Serum sample. Proteins in the serum of the blood are examined to look for features of liver disease (a test known as the ‘liver function test’ (LFT)). In addition to the LFT there is a wide range of other less commonly performed serum tests that are used to help diagnose particular digestive diseases.
Visualisation of the digestive tract
X-ray studies are also used in the investigation of digestive disease. Because the soft tissue of the bowel is not clearly exposed by X-ray imaging, a liquid mixture containing the salt barium sulphate is used to provide ‘contrast’ between the hollow space within the bowel and the surrounding soft tissues (as the metal of barium shows up as white on X-ray images). In the procedure called ‘barium swallow’, the patient is requested to drink a liquid containing barium sulphate. As the liquid lines the upper digestive tract, X-ray images will reveal its outline and show up areas of muscle spasm, ulcers or tumours. Figure 3.1b-II is a clear barium-swallow X-ray image, in this case depicting an oesophageal cancer. The white area shows the internal shape of the oesophagus, and the arrows indicate the narrowing caused by the tumour.
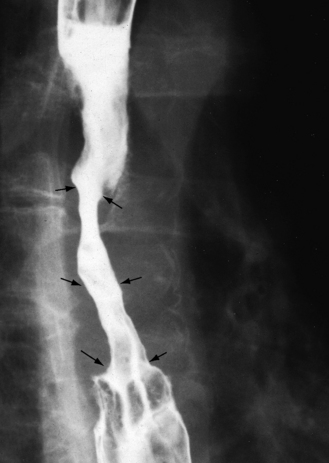
Figure 3.1b-II • A barium-swallow image, showing a carcinoma of the oesophagus (narrowing by tumour indicated by arrows).
The endoscope can also be used to pass a fine tube into the pancreatic duct and bile ducts. Barium can be injected up this tube so that X-ray images can show up the delicate internal structure of the pancreas and the gallbladder. This procedure is known as ‘endoscopic retrograde cholangiopancreatography’ (ERCP). Figure 3.1b-III illustrates an image taken during an ERCP. The thick white curved tube in this image is the end of the endoscope.
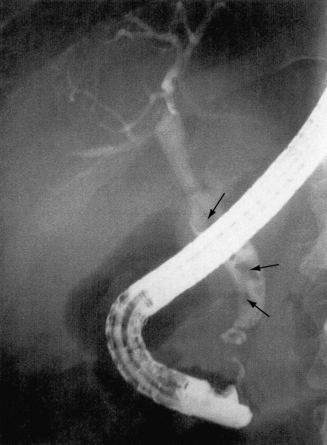
Figure 3.1b-III • An ERCP image from a patient with gallstones
•Several stones can be seen within the dilated common bile duct (arrows).
 Self-test 3.1b The investigation of the gastrointestinal system
Self-test 3.1b The investigation of the gastrointestinal system
1. A patient of yours is seen by a gastroenterologist who suspects possible stomach cancer. What investigations do you think this patient might have to undergo?
2. A patient has epigastric pain. Which organs might be involved?
3. A patient has a swelling in the right iliac fossa. Which organs might be involved?
Answer
1. The patient will first have to undergo a physical examination. If the patient has stomach cancer, the examining doctor might find the following signs:
2. Epigastric pain could signify a problem with the lower oesophagus, stomach, duodenum, pancreas or heart.
3. A lump in the right iliac fossa could signify a possible problem in the appendix, ureter, caecum, fallopian tube or ovary.
radiofrequency fields, but these currently are considered to carry little risk. However, an abdominal CT scan exposes the patient to over 50 times the amount of radiation associated with a chest X-ray, and so its use has to be guided on the basis that the potential benefits of the information outweigh the risks of carcinogenesis (cancer formation) from radiation exposure.
Chapter 3.1c Diseases of the mouth, oesophagus, stomach and duodenum
Introduction
To help with progression along this journey of diseases of each part of the gastrointestinal tract, it may be useful to be reminded first of the physiological descriptions to be found in the relevant sections in Chapter 3.1a (see Q3.1c-1).
Important diseases of the mouth and salivary glands
Mouth ulcers
Less commonly, mouth ulcers may be part of a more severe digestive condition. The lower gastrointestinal diseases of Crohn’s disease, ulcerative colitis and coeliac disease are all associated with mouth ulceration. These conditions are studied in more detail in Chapter 3.1e.
 Information Box 3.1c-I
Information Box 3.1c-ICold sores
The nature of infection by the herpes simplex virus (HSV) in the causation of cold sores was introduced in Chapter 2.4a by means of an example of the pathology of infectious diseases. First infection by HSV may cause a crop of painful ulcers. After this the virus remains ‘latent’ in a nerve cell, and characteristic symptoms of the painful crusting and weeping cold sore may reoccur at times of stress or exposure to extreme sunlight.
The same virus may also cause genital herpes infections. Oral sex can lead to the transmission of an oral cold sore to the genitalia of the sexual partner (for more detail on genital herpes; see Chapter 5.2d).
 Information Box 3.1c-II
Information Box 3.1c-IIOral thrush (candidiasis)
Overgrowth of the Candida yeast (thrush) is described in Chapter 2.4b. Overgrowth of the Candida yeast in the mouth (oral thrush) appears as white patches on the tongue and lining of the mouth, and may or may not be painful. Thrush of the oesophagus can result in difficult and painful swallowing. Thrush of the oesophagus is a common first feature of the progression of human immunodeficiency virus (HIV) infection to acquired immune deficiency syndrome (AIDS).
 Information Box 3.1c-III
Information Box 3.1c-III Information Box 3.1c-IV
Information Box 3.1c-IV Information Box 3.1c-V
Information Box 3.1c-VSalivary gland infections (sialadenitis)
There are three pairs of major salivary glands (see Chapter 3.1a). The parotid glands hug the posterior border of the masseter muscle on the face, the submandibular glands sit under the inferior edge of the lower jaw bone (mandible), and the sublingual glands sit under the tongue. All are exocrine glands and release their secretions via ducts into the mouth cavity.
 Information Box 3.1c-VI
Information Box 3.1c-VI Information Box 3.1c-VII
Information Box 3.1c-VII
 Information Box 3.1c-VIII
Information Box 3.1c-VIIIThe red flags of diseases of the mouth
Some patients with diseases of the mouth will benefit from referral to a conventional doctor for assessment and/or treatment. Red flags are those symptoms and signs that indicate that referral is to be considered. The red flags of the diseases of the mouth are described in Table 3.1c-I. This table forms part of the summary on red flags given in Appendix III, which also gives advice on the degree of urgency of referral for each of the red flag conditions listed.
Table 3.1c-I Red Flags 4 – diseases of the mouth
| Red Flag | Description | Reasoning |
|---|---|---|
| 4.1 | Persistent oral thrush (candidiasis) (appearing as a thick, white coating on the tongue or palate) | Although common in the newborn, oral thrush in children and adults is not a normal finding, and merits referral to exclude an underlying cause. Common causes include corticosteroid use (including asthma inhalers), diabetes, immunodeficiency (including HIV/AIDS) and cancer. Dentures in elderly people can also predispose to oral thrush |
| 4.2 | Persistent painless white plaque (leukoplakia) (appearing as a coat that appears to sit on the surface of the sides of the tongue) | Leukoplakia is a precancerous change that signifies an increased risk of mouth cancer. It is more common in smokers and in those with a high alcohol intake. A particular form of leukoplakia is also associated with HIV/AIDS Early treatment of leukoplakia can prevent invasive mouth cancer, so referral is merited |
| 4.3 | Painless enlargement of a salivary gland over weeks to months | This needs referral to exclude salivary gland cancer, which is most common in people over the age of 60 years |
| 4.4 | Painful or painless enlargement of a salivary gland immediately after eating | This suggests a salivary gland stone or obstruction from dried secretions. Early treatment is to maximise hydration by encouraging drinking, and to encourage salivation (e.g. with lemon juice). If the problem is persistent, referral is recommended, as surgical removal of the stone may be necessary |
| 4.5 | Tender or inflamed gums or salivary glands which do not respond within days to your treatment | May be accompanied by fever or malaise. These symptoms suggest dental abscess or infection of a salivary gland, and if they persist indicate a need for referral for antibiotic treatment to prevent inflammatory damage to the dental roots or salivary glands |
| 4.6 | Ulceration of the mouth if persistent (for more than one week) or if preventing proper hydration | The most common cause of painful ulceration of the mouth is herpes simplex. This can be so severe as to inhibit drinking in a child. If this is the case, the child may need to be hospitalised for rehydration If ulceration persists for over 2 weeks this might suggest an underlying inflammatory condition (e.g. Crohn’s disease) or mouth cancer, which will require further investigation Rarely, severe mouth ulceration can be the first sign of bone marrow failure (see Red Flags A1, in Appenix III), and in this case results from a very low white blood cell count Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
