generating motion in three planes, with predominance of the planes of motion in function of the magnitude of the corresponding vectorial component.
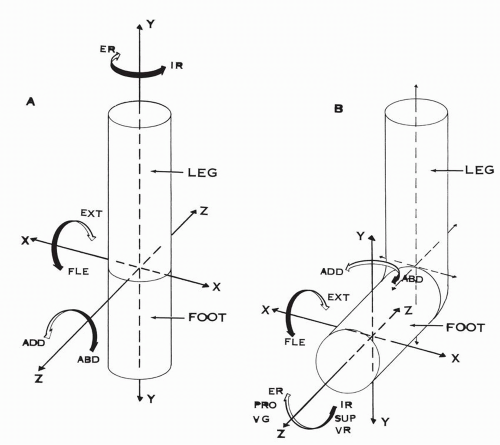 Figure 10.1 (A) Axes of motion in the foot and leg of the embryo: the foot is aligned with the leg. (B) Axes of motion in the fetus with the foot at right angle to the leg. (ER, external rotation; IR, internal rotation; EXT, extension; FLE, flexion; ABD, abduction; ADD, adduction; PRO, pronation; SUP, supination; VG, valgus; VR, varus.) The vertical axis of ER, IR of the leg is now the longitudinal axis of ER, IR of the foot. The longitudinal axis of ABD, ADD of the leg is now the vertical axis of ABD, ADD of the foot. The transverse axis of FLE, EXT remains unchanged. |
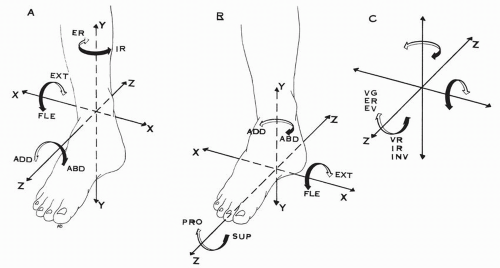 Figure 10.2 (A) Axes of motion of the ankle and leg. YY axis of ER, IR of the leg-talus. XX′ axis of FLE, EXT of the talus. ZZ axis of ASD, ADD of the talus. (B) Axes of motion of the foot plate. YY axis of ADD, ABD, XX axis of FLE, EXT. ZZ axis of SUP, PRO. (C) Different terminology used for the motion around the longitudinal axis ZZ, VG, ER, EV and VR, IR, INV. (ER, external rotation; IR, internal rotation; FLE, flexion; EXT, extension; ASD, abduction; ADD, adduction; VG, valgus; VR, varus; EV, eversion; INV, inversion.) |
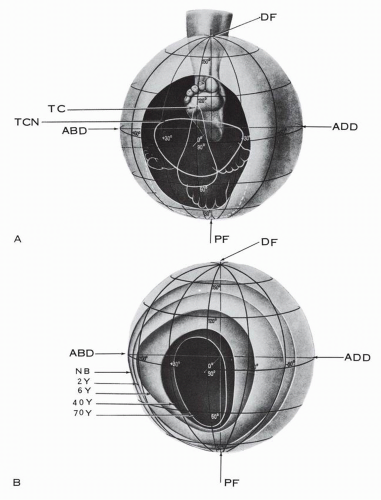 Figure 10.3 Field of motion of the foot-ankle complex. With aging, there is transverse constriction of the field of motion. (A) Oval contour of the field of motion. (B) Field of motion in different age groups. (TC, field contribution of talocrural joint; TCN, field contribution of talocalcaneonavicular joint; DF, dorsiflexion; PF, plantar flexion; ABD, abduction; ADD, adduction; NB, newborn; 2Y, 2 years old; 6Y, 6 years old; 40Y, 40 years old; 70Y, 70 years old.) (Adapted from Lang J, Wachsmuth W. Praktische Anatomie: Ein Lehr- und Hilfsbuch der anatomischen Grundlagen ärztlichen Handelns, Vol 1, Part 4. Berlin: Springer-Verlag; 1972:370.) |
The functional capacity of the foot and ankle is age dependent. The functional field is the largest in the newborn and it gradually constricts with aging, more in the transverse segment than in the vertical. At age 2 to 6 years, the field is transversely oval; at age 40 it is converted into a high oval; and, by age 70, it is narrow, limited mainly to the vertical segment.8 In terms of functional capacity, the foot at age 70 years can dorsiflex and plantarflex but has a limited capacity to adapt to walking on uneven ground.
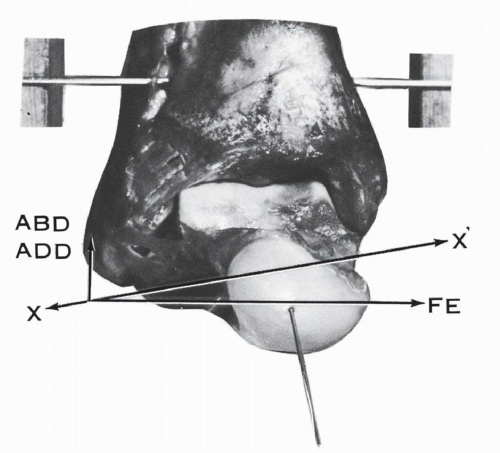 Figure 10.4 Axis of the ankle joint. The axis of the ankle joint XX is inclined as indicated and has two vectorial components: the major transverse component, which generates the motion of flexion-extension (FE), and the lesser vertical component, which generates the motion of the abduction-adduction (ABD-ADD). |
position of the talus (Figs. 10.8 and 10.9). Barnett and Napier11 based their conclusions on the determination of the curvatures of the lateral and medial marginal profiles of the talar trochlea. The center of the curvature being the axis of motion, the lateral profile is “almost always an arc of a true circle and in all positions of the talus the axis of rotation must pass through the center of this circle.’11 The medial profile is formed by the arcs of two circles with different radii. The arc of a small circle, occupying the anterior one third of the medial profile, corresponds to the dorsiflexion arc; the center of the circle is high in location. The arc of a large circle, occupying the posterior two thirds of the medial profile, corresponds to the plantar flexion arc; the center of the circle is low in location.
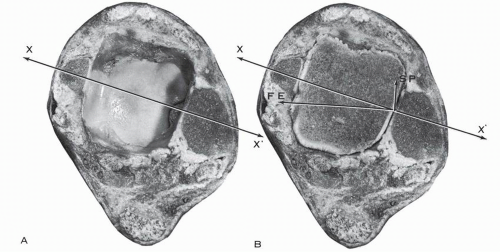 Figure 10.5 Cross-section of the ankle 2 cm above the tip of the medial malleolus, indicating the oblique orientation of the axis of motion of XX′ of the ankle in the transverse plane. The axis XX has a major transverse component for flexion-extension (FE) and a minor longitudinal component for supination-pronation (SP). (A) Cross-section demonstrating the two malleoli and the tibial plafond. (B) Cross section with the dome of the talus lodged in the ankle mortise. |
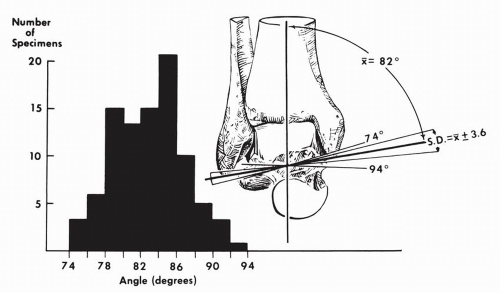 Figure 10.6 Variations in the angle between the midline of the tibia and the empirical axis of the ankle. This histogram reveals a considerable spread of individual values. (Inman TV. The Joints of the Ankle. Baltimore: Williams & Wilkins; 1976:27.) |
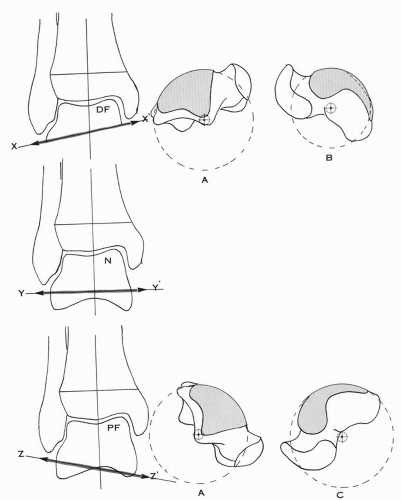 Figure 10.7 Ankle joint axis variation. In dorsiflexion (DF), the axis of motion XX′ is inclined downward and laterally. In plantar flexion (PF), the axis of motion ZZ′ is inclined downward and medially. Near neutral (N), the axis of motion YY′ is almost horizontal. The lateral trochlear contour (A) is an arc of a true circle. The medial trochlear contour is more complex. Its anterior third or dorsiflexion arc (B) belongs to a smaller circle as compared with the posterior two thirds or plantar flexion arc (C), which belongs to a large circle. (Adapted from Barnett CJ, Napier JR. The axis of rotation at the ankle joint in man: Its influence upon the form of the talus and the mobility of the fibula. J Anat. 1952;86:1.) |
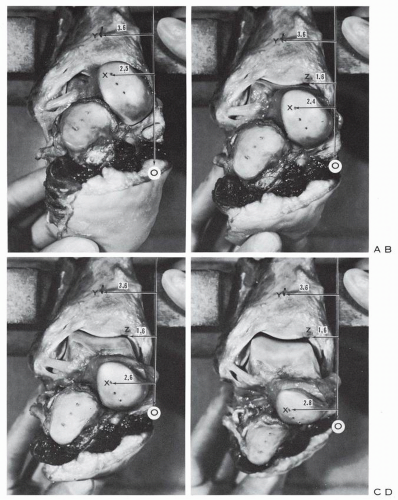 Figure 10.8 Ankle and hindfoot specimen. Tibia and fibula are stabilized. The talus is carried from dorsiflexion (A) to neutral (B) and plantar flexion (C,D). A vertical reference line O is traced. The distance of the tibial reference points Y and Z from the line O remains constant (3.6 cm and 1.6 cm). A drill point X is taken as a reference point on the talar head. The distance from point X to the vertical reference line O is measured in all four positions: dorsiflexion distance, 2.5 cm; neutral distance, 2.4 cm; plantar flexion distance, 2.6 cm; maximum plantar flexion distance, 2.8 cm. The data indicate that, in this specimen, during dorsiflexion the talus is displaced upward and laterally around an oblique axis inclined downward and laterally. In neutral the axis is transverse, whereas in plantar flexion the axis is inclined downward and medially as the talar reference point is displaced downward and laterally. |
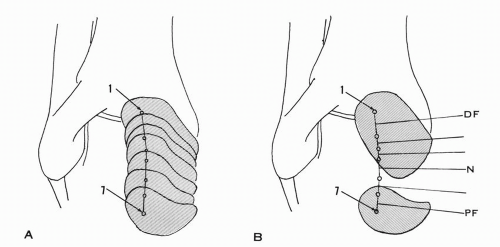 Figure 10.9 (A) Tracings of the displacements of the talar head reference point from dorsiflexion (1) to plantar flexion (7). (B) Motion axes drawn, perpendicular to the displacement lines. The axis is inclined laterally and downward in dorsiflexion and medially and downward in plantar flexion. The changeover in direction occurs very close to the neutral position of the ankle. (DF, dorsiflexion; N, neutral; PF, plantar flexion.) |
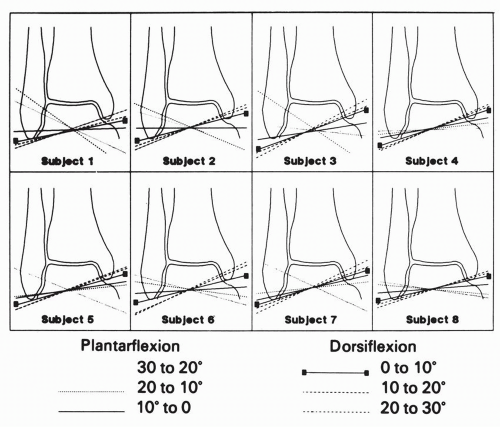 Figure 10.10 Discrete helical axes of the talocrural joint of each subject from each 10-degree interval from 30 degrees of plantar flexion to 30 degrees of dorsiflexion projected onto a coronal plane. All plantar flexion axes are more horizontal, or inclining downward and medially, than are the dorsiflexion axes. (Lundberg A, Svensson OK, Nemeth G, et al. The axis of rotation of the ankle joint. J Bone Joint Surg Br. 1989;71 [1]:94.) |
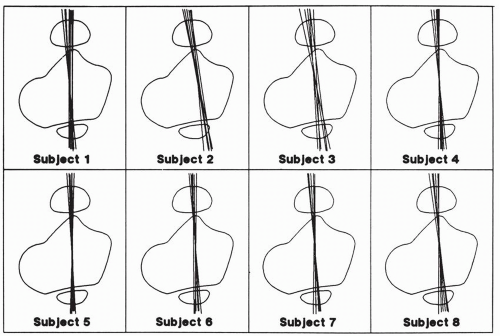 Figure 10.11 Discrete helical axes of the talocrural joint projected onto a horizontal plane. Axes tend to fall parallel to a transverse plane through the malleoli. (Lundberg A, Svensson OK, Nemeth G, et al. The axis of rotation of the ankle joint. J Bone Joint Surg Br. 1989;71 [1]:94.) |
of plantar flexion and dorsiflexion of the ankle.17 The markings were not parallel and converged toward a point 10.6 to 12.7 cm (4 to 5 inches) medial to the ankle joint and the talar trochlea offered at any time to the bimalleolar fork not the transverse dimension but a larger and constant generating line of the truncated cone (Fig. 10.17). The potential play of the talus in plantar flexion is thus absent.
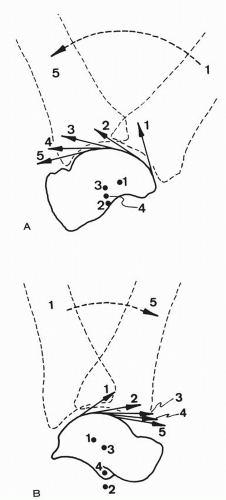 Figure 10.12 Instant centers of rotation and surface velocities from plantar flexion (1) to dorsiflexion (5) in the ankle. (A) Nonweight-bearing: the instant centers of rotation are located in the talus. The surface velocities indicate joint distraction at the beginning of motion, followed by sliding. (B) Weight bearing: an instant center of rotation may be located below the talus. The surface velocities indicate also distraction, followed by sliding. Compression or jamming may occur in maximum dorsiflexion. (Sammarco JG, Burstein AH, Frankel VH. Biomechanics of the ankle: A kinematic study. Orthop Clin North Am. 1973;4[1]:75.) |
TABLE 10.1 REPORTED NORMAL RANGES OF ANKLE JOINT MOTION | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
the tibia. The inferior peroneo-tibial ligaments are relaxed and the synovial fringe is expulsed from the peroneo-tibial interval and appears in the external angle of the mortise.
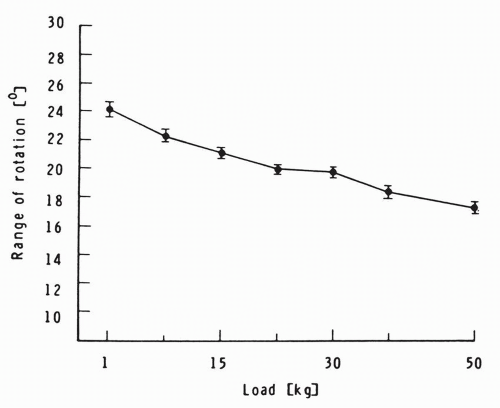 Figure 10.13 Mean range of horizontal talar medial rotation with a rotary torque of 3 N*m under variable degrees of vertical load. The horizontal talar rotation decreases with increased vertical load. (McCullough CJ, Burge PD. Rotary stability of the load-bearing ankle. An experimental study. J Bone Joint Surg Br. 1980;62[4]:460.) |
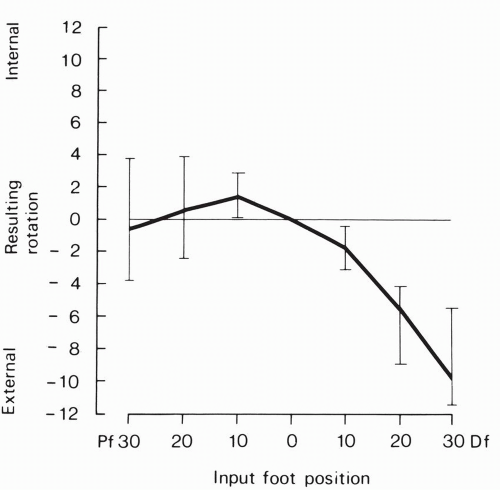 Figure 10.14 Horizontal rotation of the talus around the vertical axis at different dorsiflexion-plantar flexion input of the ankle-foot. (Lundberg A, Goldie I, Kalin BO, et al. Kinematics of the ankle/foot complex. Plantar flexion and dorsiflexion. Foot Ankle. 1989;9[4]:194.) |
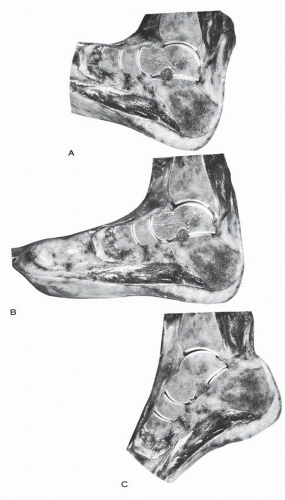 Figure 10.15 Sagittal cross-section of the hindfoot, indicating that in (A) full dorsiflexion, (B) neutral position, and (C) full plantar flexion, the articular surface of the tibia covers two thirds of the talar articular surface. At no time in plantar flexion is the narrower posterior third of the talus occupying the entire ankle mortise. |
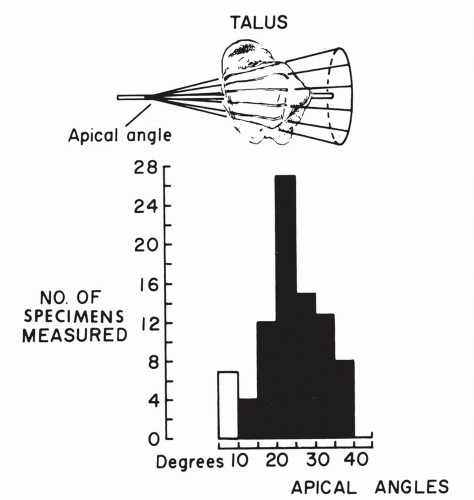 Figure 10.16 Variations of the apical angles of the conical surface of the talar trochlea obtained by extending directions of saw cuts toward the medial side. (Inman TV. The Joints of the Ankle. Baltimore: Williams & Wilkins; 1976:23.) |
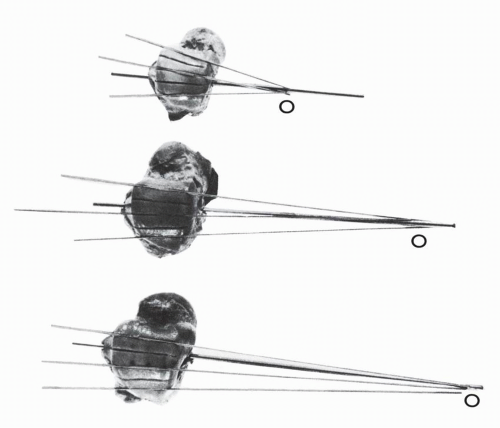 Figure 10.17 The trochlear surface of the talus is a truncated cone. The talus is carried from full dorsiflexion to full plantar flexion, and at each interval a saw cut is made on the trochlear surface along the anterior tibial articular margin. The serial saw cuts are not parallel but converge to the apex O of the cone, as demonstrated in the three tali. (Inman TV. The Joints of the Ankle. Baltimore: Williams & Wilkins; 1976:21.) |
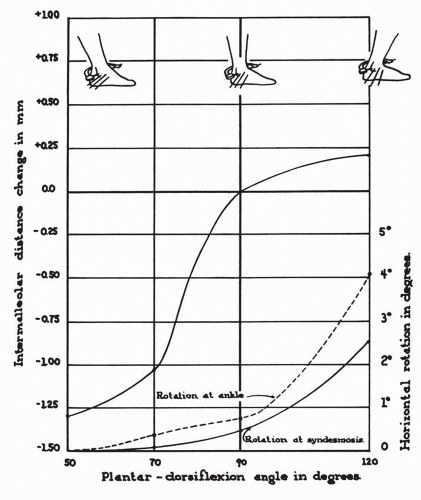 Figure 10.18 Rotation at the ankle and at the syndesmosis and the changes in the intermalleolar distance on dorsiflexion of the foot. (Close JR. Some applications of the functional anatomy of the ankle joint. J Bone Joint Surg Am. 1956;38[1]:771.) |
additional sectioning of the posterior tibiofibular ligament, the total diastasis was 7.3 mm (range, 3.0 to 15.5 mm). The findings with regard to the degree of rotation paralleled those regarding distasis. The mean external rotation increased 2.7 degrees after the anterior tibiofibular ligament was cut. The mean total increase in rotation was 10.2 degrees when all three ligaments were sectioned.
TABLE 10.2 CONTACT AREAS IN INTACT SPECIMENS | |||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||
patterns of response to position of the ankle. On the medial side, there was a relatively constant force throughout plantar flexion, up to roughly 5 degrees of dorsiflexion. From there on, there was a rapid decrease in force. Laterally, tibiotalar forces gradually increased as the ankles moved from extreme plantar flexion to 5 degrees of dorsiflexion.” With further dorsiflexion, the response to force flattened out (Figs. 10.19, 10.20, 10.22).
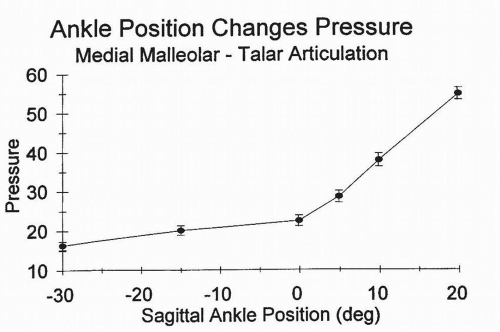 Figure 10.19 Change in force at the medial malleolar-talar articulation as a function of sagittal position of the ankle as measured by force transducers secured to the midpoint of the medial malleolar articular surface. The ankle specimen is axially loaded in neutral and cycled through a sagittal range of motion. (From Michelson JD, Checcone M, Kuhn T, et al. Intra-articular load distribution in the human ankle joint during motion. Foot Ankle Int. 2003;3:226-233, Fig. 5.) |
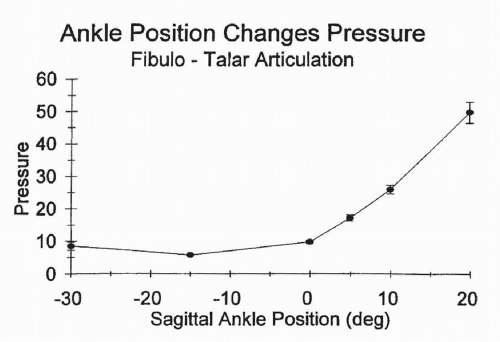 Figure 10.20 Change in force at the lateral malleolar-talar articulation as a function of sagittal position of the ankle as measured by force transducers secured to the midpoint of the lateral malleolar articular surface. The ankle specimen is axially loaded in neutral and then cycled through a sagittal range of motion. (From Michelson JD, Checcone M, Kuhn T, et al. Intra-articular load distribution in the human ankle joint during motion. Foot Ankle Int. 2003;3:226-233, Figure 6.) |
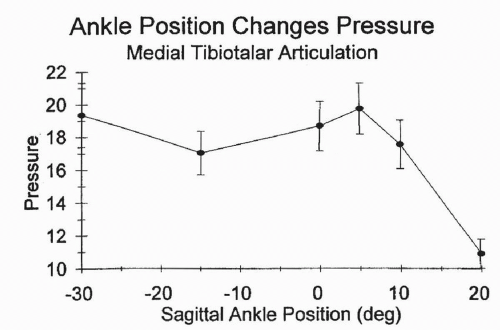 Figure 10.21 Change in force at the medial talar dome tibial plafond articulation as a function of sagittal position of the ankle as measured by force transducers secured to the midpoint of the articular surface of the medial plafond. The ankle specimen is axially loaded in neutral and cycled through a sagittal range of motion. (From Michelson JD, Checcone M, Kuhn T, et al. Intra-articular load distribution in the human ankle joint during motion. Foot Ankle Int. 2003;3:226-233, Fig. 7.) |
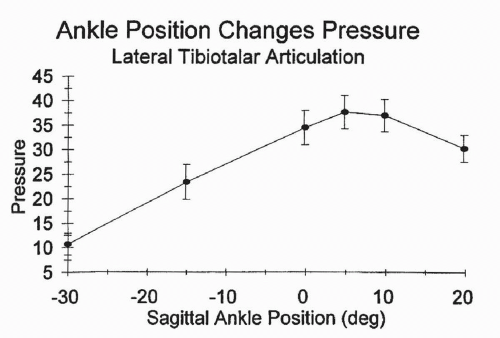 Figure 10.22 Change in force at the talar dome tibial plafond articulation as a function of sagittal position of the ankle as measured by force-transducers secured to the midpoint of the articular surface of the lateral plafond. The ankle specimen is axially loaded in neutral and then is cycled through a sagittal range of motion. (From Michelson JD, Checcone M, Kuhn T, et al. Intra-articular load distribution in the human ankle joint during motion. Foot Ankle Int. 2003;3:226-233, Figure 8.) |
the flexor digitorum longus tendon, the flexor hallucis longus tendon, and their fibrous sheaths contribute to stability.
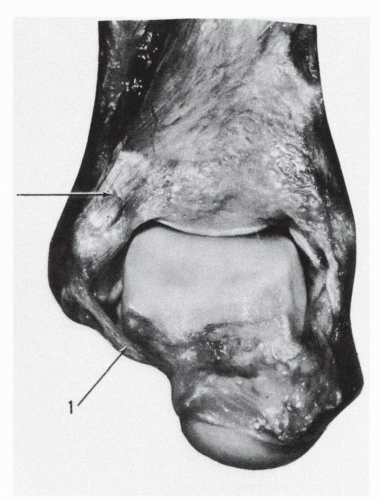 Figure 10.23 In marked plantar flexion the anterior talofibular ligament (1) braces the talus and makes a turn around the anterolateral corner of the talar body. |
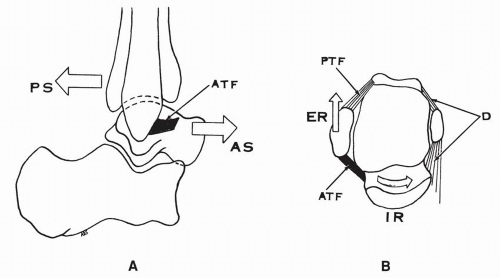 Figure 10.24 Function of the anterior talofibular ligament (ATF). (A) ATF ligament limits the anterior shift of the talus or the posterior shift of the tibia-fibula. (B) ATF ligament limits the internal rotation of the talus or the external rotation of the fibula. (ATF, anterior talofibular ligament; PTF, posterior talofibular ligament; D, deltoid ligament; AS, anterior shift; PS, posterior shift; IR, internal rotation of the talus; ER, external rotation of the fibula.) |
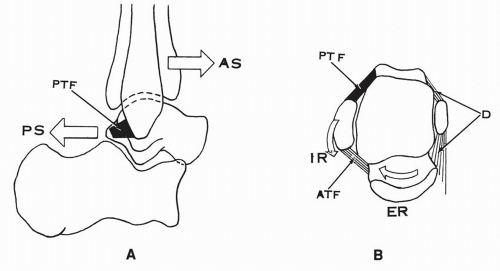 Figure 10.25 Function of the posterior talofibular ligament (PTF). (A) PTF limits the posterior shift of the talus or the anterior shift of the fibula-tibia. (B) PTF limits the external rotation of the talus or the internal rotation of the fibula. (PTF, posterior talofibular ligament; ATF, anterior talofibular ligament; D, deltoid ligament; PS, posterior shift of the talus; AS, anterior shift of the tibia-fibula; ER, external rotation of the talus; IR, internal rotation of the fibula.) |
ligament is taut in plantar flexion and less tense in dorsiflexion (Fig. 10.27), whereas in others the tension in this ligament remains constant in all positions.
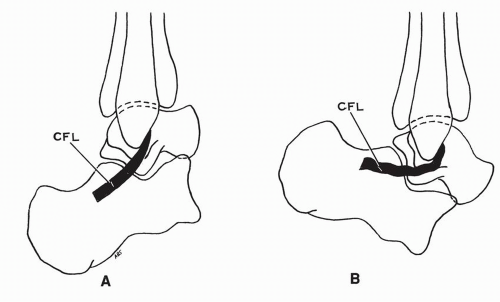 Figure 10.26 Tension in calcaneofibular ligament (CFL). (A) CFL taut in dorsiflexion of ankle. (B) CFL relaxed in plantar flexion of ankle. |
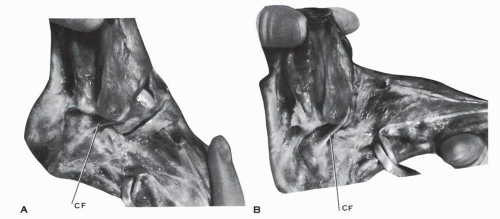 Figure 10.27 In this anatomic specimen of the ankle, the calcaneofibular ligament (CF) is taut in plantar flexion (A) and less tense in dorsiflexion (B). |
ligament, of the ankle joint, and prevents the talar tilt of the talus. In plantar flexion, the anterior talofibular ligament is vertical and functions as a collateral ligament, stabilizing the talus laterally. The average angle between the two ligaments, measured in their projection on the sagittal plane, is 105 degrees ± 24 degrees.10 The reciprocal arrangement of the two ligaments is efficient if the angle between the two ligaments is 90 degrees. A horizontal calcaneofibular ligament does not provide the same stability.
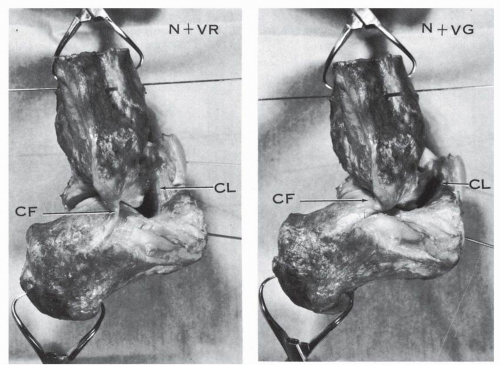 Figure 10.28 Hindfoot specimen, lateral view. The ankle is held in neutral position (N) and the os calcis is moved into varus (VR) or valgus (VG). In varus the calcaneofibular ligament is relaxed and the cervical ligament is vertical and tense. In valgus the calcaneofibular ligament is taut and the cervical ligament is oblique or horizontal but still tense. (CF, calcaneofibular ligament; CL, cervical ligament.) |
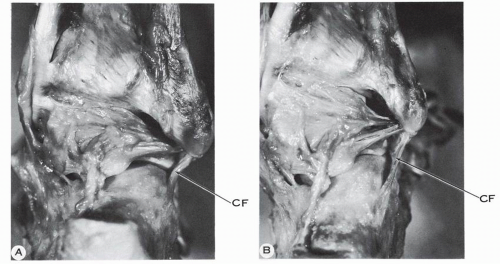 Figure 10.29 Hindfoot specimen, posterolateral view. The ankle is held in neutral. (A) The heel is in varus and the calcaneofibular ligament (CF) is relaxed. (B) The heel is in valgus and the calcaneofibular ligament is taut. |
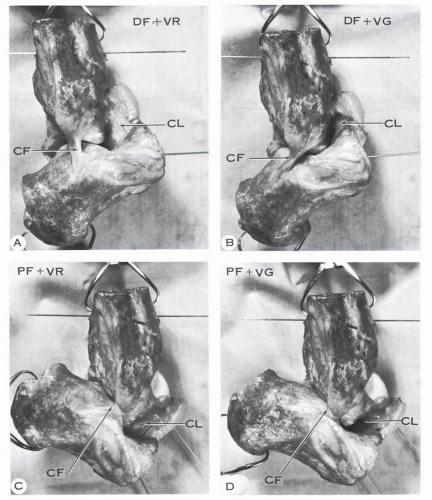 Figure 10.30 Hindfoot specimen, lateral view, in dorsiflexion (DF) and plantar flexion (PF) combined with varus (VR) or valgus (VG) of the os calcis. The dorsiflexion and plantar flexion are indicated by the K-wires implanted in the talus and the os calcis. The valgus and varus are recognized by the relative position of the talus and os calcis: in varus the lateral talar process is away from the posterolateral corner of the sinus tarsi, whereas in valgus the same process strikes or is very close to the sinus tarsi of the os calcis. (A) Combination of dorsiflexion and varus. (B) Combination of dorsiflexion and valgus. The calcaneofibular ligament is taut, more so in valgus. (C) Combination of plantar flexion and varus. (D) Combination of plantar flexion and valgus. In (C) and (D) the calcaneofibular ligament is less taut than in A and B, yet slightly more tension is present in the ligament in valgus. The cervical ligament (CL) is nearly vertical and parallel to the calcaneofibular ligament in dorsiflexion of the ankle and varus of the heel. The cervical ligament is taut in both valgus and varus. |
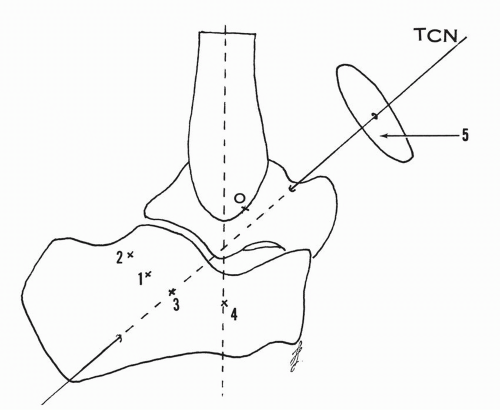 Figure 10.31 Hindfoot, lateral view. O indicates the origin of the calcaneofibular ligament and the numbers 1 to 4 the calcaneal insertion of the same ligament. The variable insertion determines the obliquity of the ligament; 1, common insertion, oblique ligament; 2, horizontal ligament; 3, ligament located along the projection of the talocalcaneonavicular axis (TCN); 4, vertical ligament. The displacement of the insertional points 1 to 4 is along arcs of circles parallel to the circle 5, which is perpendicular to the talocalcaneonavicular axis. |
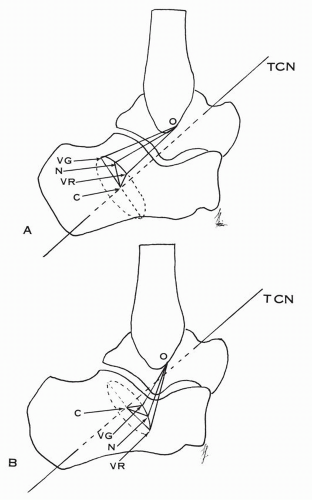 Figure 10.32 Calcaneofibular ligament with common insertion. (A) O indicates the origin of the ligament and N the insertional position in neutral. In valgus (VG) and varus (VR) the displacements occur along the circle C, which is perpendicular to the talocalcaneonavicular axis (TCN). In valgus the distance from the origin to the insertion is longer and the calcaneofibular ligament is taut. In varus the distance is shorter and the ligament is more relaxed. (B) In the vertical type of calcaneofibular ligament, the distance between the origin of the ligament and its insertion is greater in varus and less in valgus. The ligament is taut in varus and relaxed in valgus. |
talofibular ligament and the calcaneofibular ligament was again confirmed. During the arc of extension-flexion, when one ligament is relaxed, the other is strained, and vice versa. This is similar to Inman’s concept of coupling of the two ligaments.
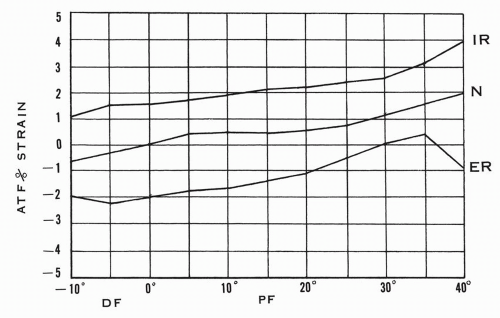 Figure 10.33 Percent strain in anterior talofibular ligament (ATF) with the foot in different degrees of plantar flexion, dorsiflexion—in neutral or combined with external-internal rotation of the foot. In the neutral position of the ankle, the internal rotation increases the strain, whereas the external rotation decreases the strain in the ligament. (Adapted from Renstrom P, Wertz M, Incavo S, et al. Strain in the lateral ligaments of the ankle. Foot Ankle. 1988;9[2]:62.) |
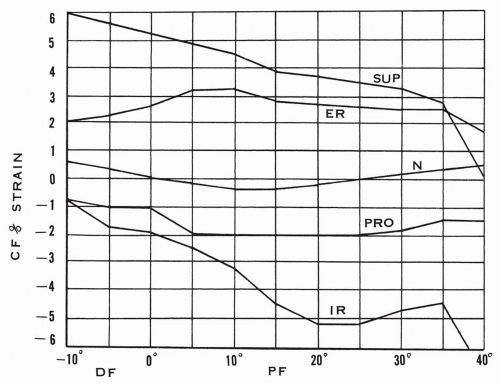 Figure 10.34 Percent strain in calcaneofibular ligament with the foot in different degrees of plantar flexion, dorsiflexion—in neutral or combined with supination-pronation or internal-external rotation of the foot. In neutral position of the ankle, the external rotation or the supination of the foot increases the strain of the ligament, whereas the pronation and the internal rotation decrease the strain. (N, neutral; SUP, supination; PRO, pronation; IR, internal rotation; ER, external rotation.) (Adapted from Renstrom P, Wertz M, Incavo S, et al. Strain in the lateral ligaments of the ankle. Foot Ankle. 1988;9[2]:62.) |
TABLE 10.3 VARIATIONS IN DEGREE OF NORMAL TALAR TILT | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 10.4 NORMAL ANTERIOR TALAR DISPLACEMENT | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||
transection of the ligament, and in dorsiflexion the increase was 5.7 degrees ±3.6 degrees, or 62%, from the initial talar rotation of 10.2 degrees ±6.7 degrees. In essence, the release of the anterior talofibular ligament increases the anteromedial shift of the talus and allows a lateral talar tilt.
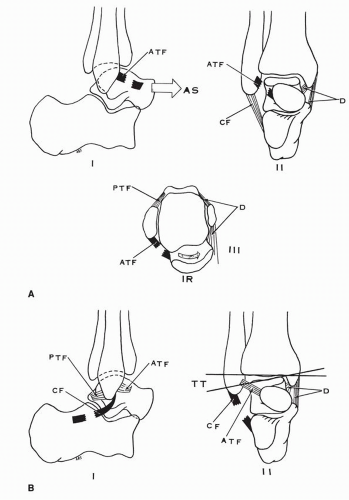 Figure 10.35 (A) The isolated tear of the anterior talofibular ligaments results in (I) anterior shift of the talus, (II) no lateral tilt of the talus with varus stress except for a minimal degree at the extreme of plantar flexion, (III) medial rotation of the talus. (B) The isolated transection of the calcaneofibular ligament results in (I) no anterior shift, (II) minor lateral talar tilt when the foot is plantar flexed. |
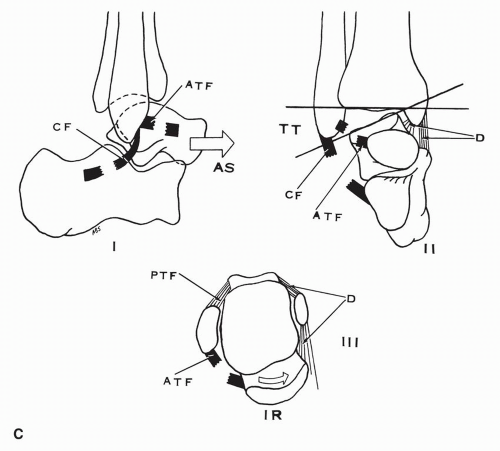 Figure 10.35 (Continued) (C) Transection of the anterior talofibular and calcaneofibular ligaments results in (I) marked anterior shift of the talus, (II) lateral talar tilt, (III) internal rotation of the talus when the foot is plantar flexed. (ATF, anterior talofibular ligament; CF, calcaneofibular ligament; PTF, posterior talofibular ligament; IR, internal rotation of talus.) (Data from Glasgow M, Jackson A, Jamieson AM. Instability of the ankle after injury to the lateral ligament. J Bone Joint Surg Br. 1980;62[2]:196.) |
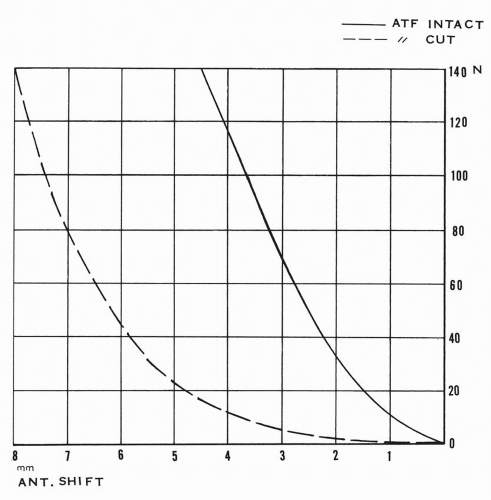 Figure 10.36 Anterior shift of the talus before and after section of the anterior talofibular ligament in dorsiflexion with variable degree of force applied. (ATF, anterior talofibular ligament; ANT shift, anterior displacement; N, Newton [force unit applied].) (Curve adapted from Johnson EE, Markolf KL. The contribution of the anterior talo-fibular ligament to ankle laxity. J Bone Joint Surg Am. 1983;65[1]:86.) |
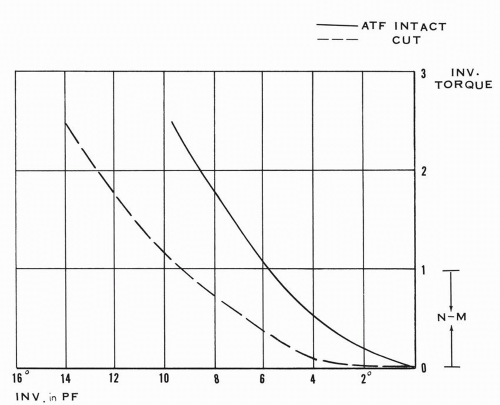 Figure 10.37 Inversion of the talus or lateral talar tilt in plantar flexion before and after section of the anterior talofibular ligament with variable inversion torque applied. (ATF, anterior talofibular ligament; INV, in PF, inversion or lateral tilt in plantar flexion; INV torque, inversion torque in N-M [Newtonmeters].) (Curve adapted from Johnson EE, Markolf KL. The contribution of the anterior talo-fibular ligament to ankle laxity. J Bone Joint Surg Am. 1983;65[1]:86.) |
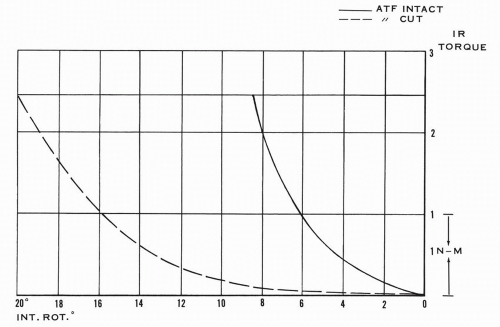 Figure 10.38 Internal rotation of the talus before and after section of the anterior talofibular ligament with variable internal rotation torque applied. (ATF, anterior talofibular ligament; INT. RCT., internal rotation of talus; IR TORQUE, internal rotational torque in N-M [Newton-meters].) (Curve adapted from Johnson EE, Markolf KL. The contribution of the anterior talo-fibular ligament to ankle laxity. J Bone Joint Surg Am. 1983;65[1]:86.) |
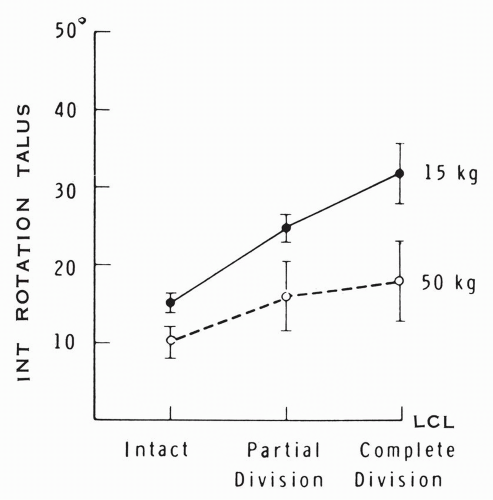 Figure 10.39 Mean range of medial talar rotation under vertical loading with lateral collateral ligament (LCL) intact, with partial division (section of the anterior talofibular ligament), and with complete division of the ligament (added section of the calcaneofibular and posterior talofibular ligaments). (McCullough CJ, Burge PD. Rotary stability of the load-bearing ankle. An experimental study. J Bone Joint Surg Br. 1980;62[4]:461.) |
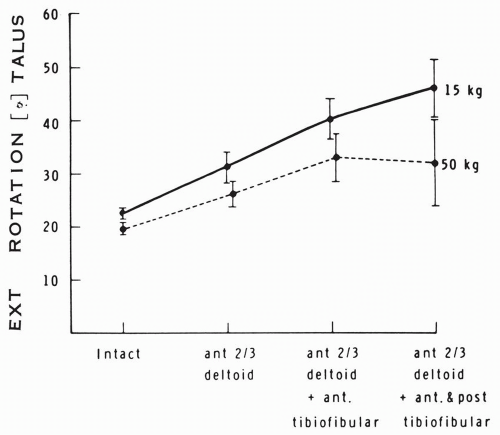 Figure 10.40 Mean range of external talar rotation under vertical loading with the ligaments intact and with sequential cuts of the anterior two thirds of the deltoid ligament and the anterior and posterior tibiofibular ligaments. (McCullough CJ, Burge PD. Rotary stability of the load-bearing ankle. An experimental study. J Bone Joint Surg Br. 1980;62[4]:461.) |
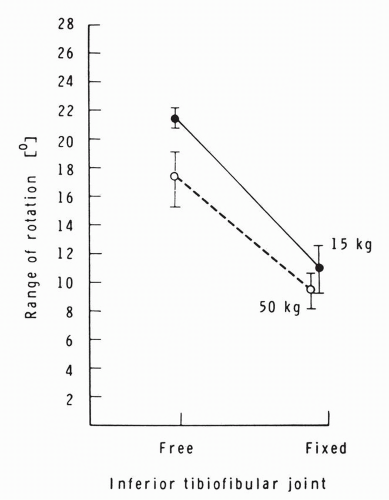 Figure 10.41 Mean range of talar external rotation under vertical load with the inferior tibiofibular joint free or fixed. (McCullough CJ, Burge PD. Rotary stability of the load-bearing ankle. An experimental study. J Bone Joint Surg Br. 1980;62[4]:402.) |
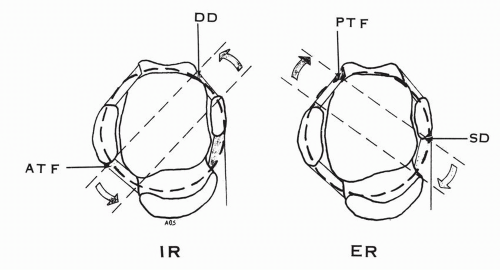 Figure 10.42 The components of the collateral ligaments of the ankle forming a ring resisting the horizontal rotation of the talus by tension in opposing pairs. Resisting the internal rotation (IR): the anterior talofibular ligament and the deep deltoid ligament. Resisting the external rotation (ER): the posterior talofibular ligament and the superficial deltoid ligament. (ATF, anterior talofibular ligament; DD, deep deltoid ligament; PTF, posterior talofibular ligament; SD, superficial deltoid ligament.) |
talus is resisted by the anterior talofibular ligament.42 This ligament is an essential component of the supportive horizontal ligamentous ring (see Fig. 10.42). The external rotation of the leg places the ligament under tension and the excess may lead to its rupture.
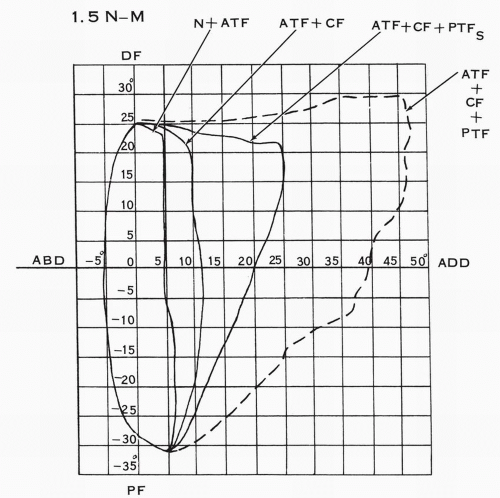 Figure 10.43 Mobility pattern in the sagittal and front planes after progressive section of the components of the lateral collateral ligament. The torque applied is 1.5 N-m. (N, neutral; ATF, anterior talofibular ligament; CF, calcaneofibular ligament; PTFS, posterior talofibular ligament short fibers; PTF, total posterior talofibular ligament; DF, dorsiflexion; PF, plantar flexion; ABD, abduction of talus; ADD, adduction of talus or lateral talar tilt.) (Adapted from Rasmussen O. Stability of the ankle joint. Analysis of the function and traumatology of the ankle ligaments. Acta Orthop Scand. 1985;56[Suppl 211]:34.) |
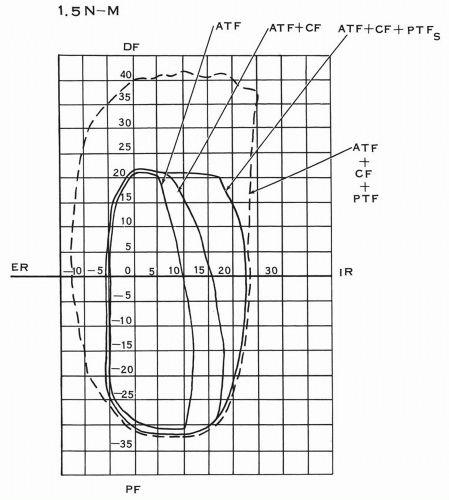 Figure 10.44 Mobility pattern in the sagittal and horizontal planes after progressive section of the components of the lateral collateral ligaments. The torque applied is 1.5 N-m. (ATF, anterior talofibular ligament; CF, calcaneofibular ligament; PTFS, short fibers of posterior talofibular ligament; ER, external rotation; IR, internal rotation; DF, dorsiflexion; PF, plantar flexion.) (Adapted from Rasmussen O. Stability of the ankle joint. Analysis of the function and traumatology of the ankle ligaments. Acta Orthop Scand. 1985;56[Suppl 211]:34.) |
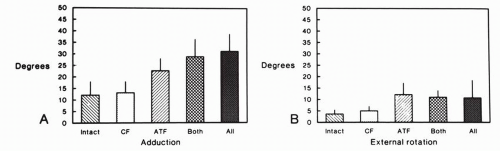 Figure 10.45 Mean maxima for adduction (A) and external rotation (B) of the tibia relative to the talus with the lateral collateral ligament intact and with sequential transection of its components. (G; calcaneofibular ligament; ATF, anterior talofibular ligament.) (Cass JR, Morrey BF, Chao EYS. Three-dimensional kinematics of ankle instability following serial sectioning of lateral collateral ligaments. Foot Ankle. 1984;5[3]:45.) |
to that of the calcaneofibular ligament. These experiments were conducted with the tested ligament oriented near vertically, which corresponds to a position of plantar flexion for the anterior talofibular ligament and a position of dorsiflexion for the calcaneofibular and the posterior talofibular ligaments.
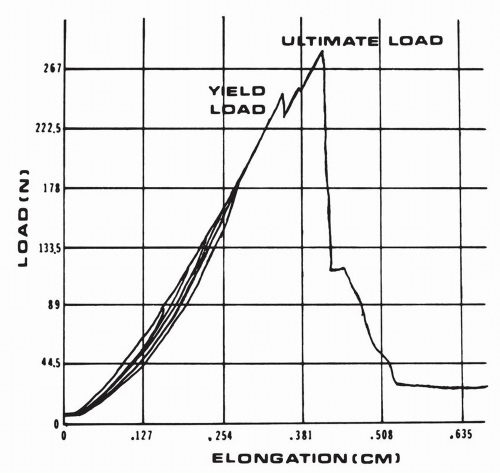 Figure 10.46 Tension-elongation results obtained from a tensile test conducted on a lateral collateral ankle ligament prepared as bone-ligament-bone. The yield point-load represents the failure of some fibers of the ligament, which is still intact. The ultimate load corresponds to the failure of the ligament. (N, Newton.) (Siegler S, Block J, Schneck CD. The mechanical characteristics of the collateral ligaments of the human ankle joint. Foot Ankle. 1988;3[5]:239.) |
of the superficial or the deep deltoid component resulted in no change in the talar lateral or anterior shift or in the medial tilt. The transection of both the superficial and deltoid ligaments resulted in a medial talar tilt or abduction of 14 degrees (range, 13 to 16 degrees) but without associated increase of the talar anterior or lateral shift (Fig. 10.48).
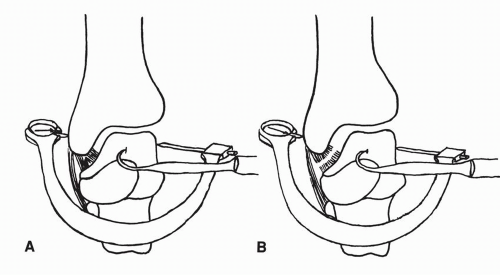 Figure 10.47 Lateral displacement of the talus after excision of the fibula and after added transection of the deep component of the deltoid ligament. (A) Talus laterally displaced 2.0 mm after removing fibula. (B) After sectioning the deep portion of the deltoid ligament 3.7 mm displacement of talus is possible. (Close JR. Some applications of the functional anatomy of the ankle joint. J Bone Joint Surg Am. 1956;38[1]:766.) |
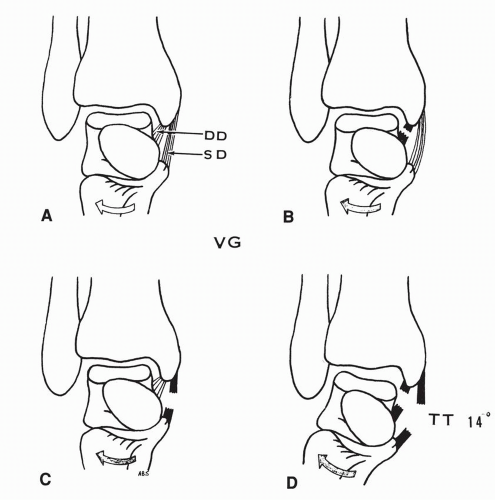 Figure 10.48 Medial talar tilt or talar abduction with valgus stress applied. (A) Superficial and deep deltoid components intact. (B) Transection of deep deltoid: no talar tilt. (C) Transection of superficial deltoid: no talar tilt. (D) Transection of both deltoid components: medial talar tilt. The lateral malleolus is intact. (SD, superficial deltoid ligament; DD, deep deltoid ligament; TT, medial talar tilt; VG, valgus stress.) (Data from Harper MC. Deltoid ligament: An anatomical evaluation of function. Foot Ankle. 1987;8[1]:19.) |
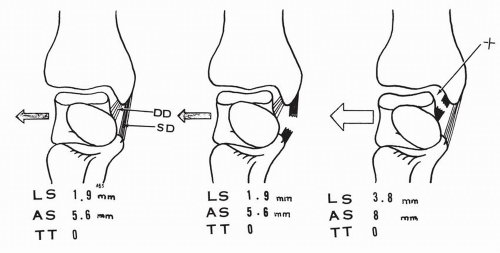 Figure 10.49 The lateral malleolus is excised. The talar lateral shift (LS), anterior shift (AS), and medial tilt (TT) are assessed with the components of the deltoid intact or with the transection of the superficial or the deep components of the deltoid ligament. The displacements are indicated in average millimeter values. (Data from Harper MC. Deltoid ligament: An anatomical evaluation of function. Foot Ankle. 1987;8[1]:19.) |
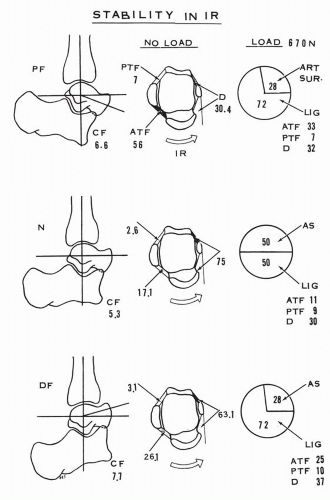 Figure 10.50 Stability of the ankle in internal rotation stress with and without vertical load of 670 N (newtons). Percentage of restraint to the internal rotation torque-displacement by each component of the collateral ligaments and the articular surfaces is presented in neutral, dorsiflexion, and plantar flexion positions of the ankle. (ATF, anterior talofibular ligament; PTF, posterior talofibular ligament; CF, calcaneofibular ligament; D, deltoid ligament; AS, articular surface; IR, internal rotation.) (Data from Stormont DM, Morrey BF, Kai-nan AN, et al. Stability of the loaded ankle. Relation between articular restraint and primary and secondary static restraints. Am J Sports Med. 1985;13[5]:295.) |
the foot on the leg without load, the calcaneofibular ligament becomes a major contributor, averaging 65% to stability. The posterior talofibular ligament is a secondary restraint. This ligament provides no resistance in 15 degrees of dorsiflexion. The deltoid ligament and the anterior talofibular ligament have secondary influences. With loading, the calcaneofibular restraint averages 43% and the posterior talofibular ligament 24%. The deltoid ligament now provides substantial support, averaging 20% except in neutral (3.2%), and the anterior talofibular ligament contributes an average of 17% to stability except in plantar flexion (5.3%). The articular surfaces under loading provide an average of 27% of stability (Fig. 10.51).
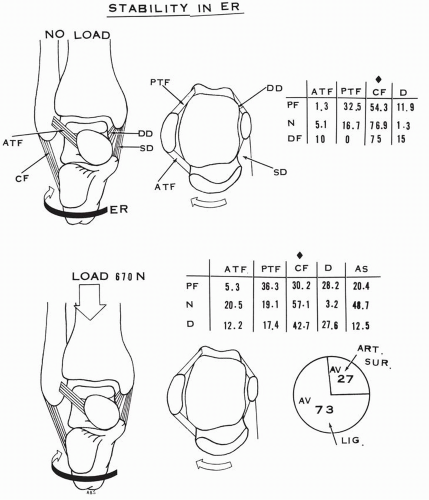 Figure 10.51 Stability of the ankle in external rotation stress with and without vertical load of 670 N (newtons). Percentage of restraint to the external rotation torquedisplacement by each component of the collateral ligaments and the articular surfaces is presented in neutral, dorsiflexed, and plantar flexed positions of the ankle. The calcaneofibular ligament is a major restraining structure. (ATF, anterior talofibular ligament; PTF, posterior talofibular ligament; CF, calcaneofibular ligament; D, deltoid ligament; AS, articular surface; AV, average contribution; ER, external rotation.) (Data from Stormont DM, Morrey BF, Kai-nan AN, et al. Stability of the loaded ankle. Relation between articular restraint and primary and secondary static restraints. Am J Sports Med. 1985;13[5]:295.) |
oriented upward, anteriorly and medially. It penetrates the posterolateral corner of the os calcis, passes perpendicular to the canalis tarsi, and pierces the superomedial aspect of the talar neck. Manter reported the angulation of the axis to have a 42 degrees average inclination (range, 29 to 47 degrees) in the sagittal plane relative to the horizontal line and a 16 degrees average medial deviation (range, 8 to 24 degrees) in the transverse plane relative to the long axis of the foot passing through the first interdigital space.50 Inman provided measurements that are very similar: 42 degrees ± 9 degrees of inclination in the sagittal plane and 23 degrees ± 11 degrees of medial deviation in the horizontal plane relative to the axis of the foot passing through the second interdigital space (Fig. 10.53).10
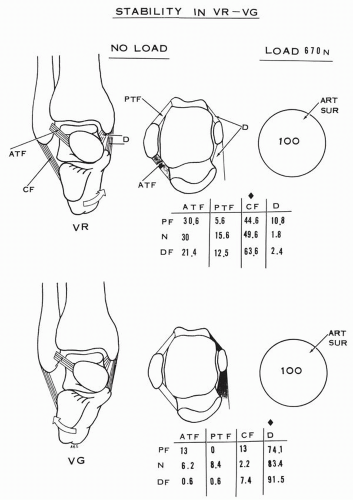 Figure 10.52 Stability of the ankle in varus and valgus stress with and without vertical load of 670 N. Percentage of restraint to the varus or valgus stress by each component of the collateral ligaments and the articular surfaces is presented in neutral, dorsiflexion, and plantar flexion of the ankle. The calcaneofibular ligament is a major restraining structure in varus stress, whereas the deltoid ligament is a major restraining structure in valgus stress of the ankle. Under vertical load the stability is provided by only the articular surfaces. (Data from Stormont DM, Morrey BF, Kai-nan AN, et al. Stability of the loaded ankle. Relation between articular restraint and primary and secondary static restraints. Am J Sports Med. 1985;13[5]:295.) |
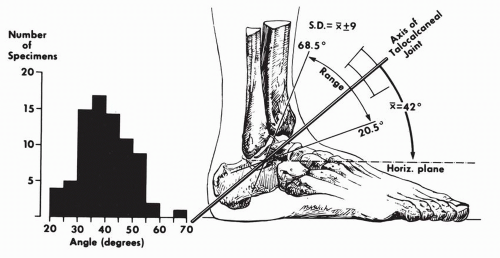 Figure 10.53 Variations in inclination of axis of subtalar joint as projected upon sagittal plane. The single observation of an angle of almost 70 degrees was present in a markedly cavus foot. (Inman TV. The Joints of the Ankle. Baltimore: Williams & Wilkins; 1976:37.) |
surface as a female ovoid surface. The combined anterior and middle calcaneal surfaces form a female ovoid surface and the inferior articular surface of the talar head forms a male more or less flattened ovoid surface. MacConaill and Basmajian analyzed the motion components generated by the moving ovoid surfaces relative to each other.30 A male ovoid surface moving on a female ovoid surface slides, rolls, and spins. The rolling is in a direction opposite to the sliding (Fig. 10.62). A female ovoid surface moving on a male ovoid surface slides, rolls or rocks, and spins. The rolling is in the direction of sliding (Fig. 10.63). The roll is a tilt that maintains the surface contact and the spin maximizes the congruency. Huson analyzed the spin at the posterior talocalcaneal joint.8 Because of the differential of the curvatures of the articular surface—more curved medially and less curved laterally—a pure sliding creates more incongruency of the corresponding surfaces, whereas an associated spin minimizes the incongruency (Fig. 10.64). This interpretation is inclusive in the broader and more comprehensive analysis of the movement of ovoid surfaces presented by MacConaill and Basmajian.30 If the ovoid surfaces are obliquely oriented with regard to the long axis of the foot, the generated motion will have two components. The associated spin creates the third motion component.
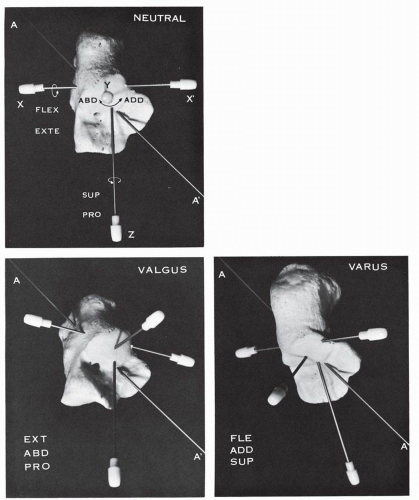 Figure 10.54 The axis of the talocalcaneonavicular joint AA′ as indicated passing through the os calcis in neutral position. The axis AA′ has three components: XX, which generates flexion-extension (FLEX-EXTE); Y, which generates abduction-adduction (ABD-ADD); Z, which generates supinationpronation (SUP-PRO). In valgus position the anterior aspect of the os calcis is simultaneously extended, abducted, and pronated. In varus position the anterior aspect of the os calcis is simultaneously flexed, adducted, and supinated. |
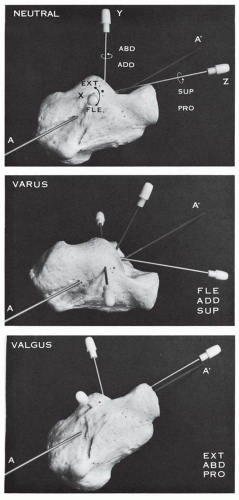 Figure 10.55 Axis of the talocalcaneonavicular joint AA′ seen in lateral view with the secondary axes X, Y, Z. The middle figure indicates the os calcis in varus and demonstrates the flexion (FLE) and supination (SUP) components. The bottom figure indicates the os calcis in valgus and demonstrates the components of extension (EXT) and pronation (PRO). (ABD, abduction; ADD, adduction.) |
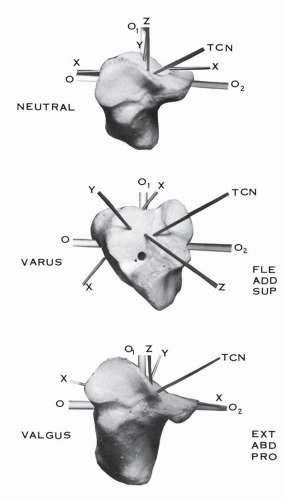 Figure 10.56 Frontal view of the os calcis. In varus of the heel the anterior aspect of the os calcis is flexed (FLE), adducted (ADD), and supinated (SUP). In valgus of the heel the anterior aspect of the os calcis is extended (EXT), abducted (ABD), and pronated (PRO). (TCN, talocalcaneonavicular axis; XX, transverse axis of flexion-extension; Y, vertical axis of abduction-adduction; Z, longitudinal axis of supination-pronation; O, O1, O2, cruciform reference line.) |
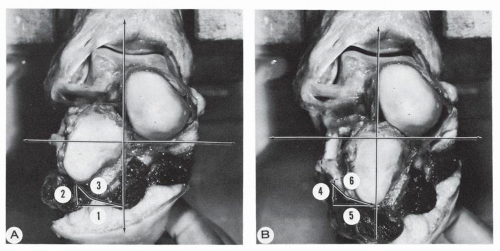 Figure 10.57 Anatomic model of the hindfoot. (A) Valgus position of the os calcis involving (1) abduction, (2) extension, (3) pronation. (B) Varus position of the os calcis involving (4) flexion, (5) adduction, (6) supination. |
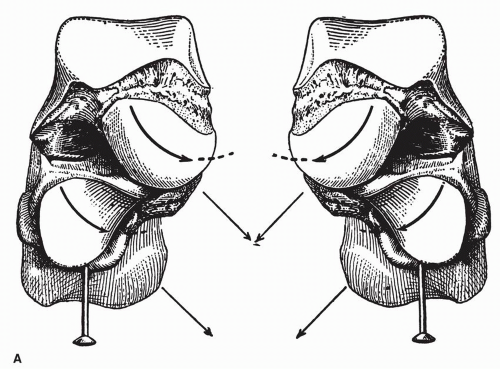 Figure 10.58 (A) Relationship of the talus and the calcaneus in the standing position as indicated by the vertical pin inserted in the calcaneus. The posterior calcaneal surface is covered by the external apophysis of the talus. The “condylar” surface of the talus is medial relative to the “trochlear” surface of the calcaneus. The long axis of the talar condylar surface is parallel to the long axis of the trochlear surface of the cuboid. Both axes are directed inferiorly, medially, and posteriorly, and this allows an “oblique flexion inwards.” |
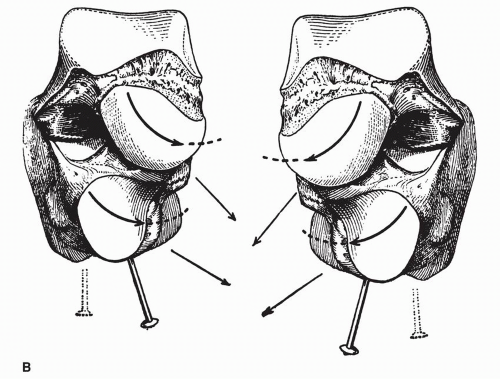 Figure 10.58 (Continued) (B) The talus has remained unchanged. The calcaneus is turned inward, as evidenced by the obliquity of the calcaneal pin. The long axes of the talar condylar and calcaneal trochlear surfaces are convergent. This corresponds to the “physiologic varus of flexion + adduction + supination,” which results from the combined movements of the navicular on the talus, the cuboid on the calcaneus, and the calcaneus on the talus. (From Farabeuf LH. Precis de Manuel Opératoire. Paris: Maisson; 1889:827.) |
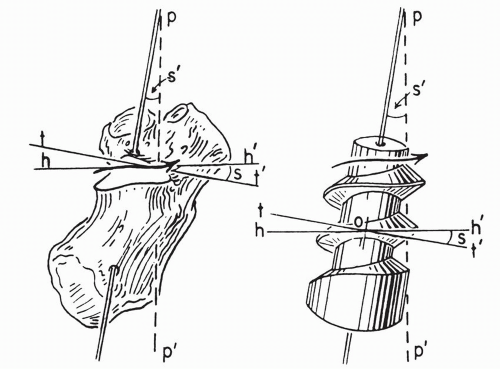 Figure 10.59 Comparison of the posterior calcaneal facet of the right subtalar joint with a right-hand screw. Arrow represents the path of a body following the screw. hh′ is the horizontal plane in which motion is occurring. tt′ is a plane perpendicular to the axis of the screw. s is the helix angle of the screw, equal to the angle s′, which is obtained by dropping a perpendicular pp′ from the axis. (Manter JT. Movements of the subtalar and transverse tarsal joints. Anat Rec. 1941;80:402.) |
 Figure 10.60 Right-hand and left-hand screws. |
TABLE 10.5 REPORTED RANGES OF SUBTALAR MOTION | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
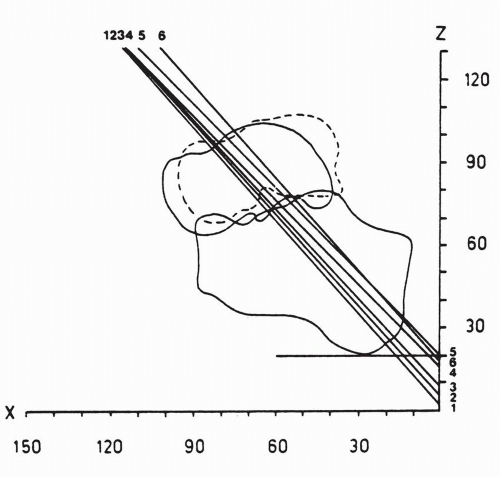 Figure 10.61 Relative talocalcaneal helical axes with 10 degrees of talocalcaneal exorotation projected on sagittal plane. (Van Langelaan EJ. A kinematical analysis of the tarsal joints. An X-ray photogrammetric study. Acta Orthop Scand. 1983;54[Suppl 204]:147.) |
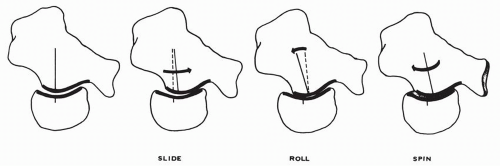 Figure 10.62 A male ovoid surface (posterior calcaneal articular surface) moving on a female ovoid surface (posterior talar articular surface) slides, rolls, and spins. The rolling is in a direction opposite to the sliding. The sliding advances the moving surface but creates a gap that is closed by the reverse rolling, and the maximum surface contact is achieved by the spinning of the moving surface. (Concept of MacConaill and Basmajian.) |
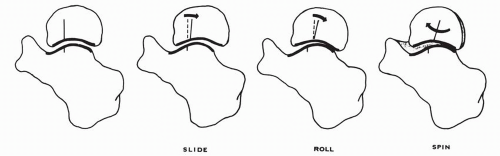 Figure 10.63 A female ovoid surface moving on a male ovoid surface slides, rolls, and spins. The rolling is in the direction of the sliding. |
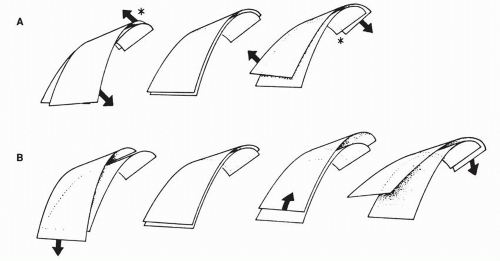 Figure 10.64 Diagrammatic representation of the posterior calcaneotalar articular surfaces. The posterior calcaneal surface has “convex profiles lying in a medial, backward and upward direction. The curvatures grow stronger in the same direction and in addition the profiles of the medial and anterior part of the facet, bordering on the canalis tarsi, are more curved than the lateral ones. Such surfaces in gliding over each other will show great discongruencies when they follow their strongest or weakest curvatures,” as seen on the lower diagrams (B). “If this shift is simultaneously combined with a turn the discongruencies are limited to a circumscribed part (indicated by the asterisk) of the articular surfaces,” as seen on the upper diagrams (A). (Huson A. Anatomical and Functional Study of the Tarsal Joints. Leiden: Drukkerij, “Luctor et Emergo”; 1961:137.) |
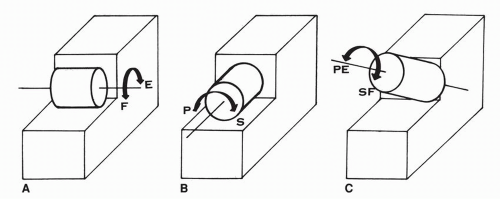 Figure 10.65 (A) A convex male surface oriented transversely generates the motion of flexion (F) and extension (E). (B) A convex male surface oriented longitudinally generates the motion of pronation (P) and supination (S). (C) A convex male surface oriented obliquely—as indicated—generates a combination of pronation-extension (PE) and supination-flexion (SF). |
talocalcaneal interosseous ligament of the canalis tarsi and the cervical ligament may be considered as cruciate ligaments of the subtalar joint, as determined by their opposite orientation. The cervical ligaments and the calcaneofibular ligament have an approximate similar orientation.
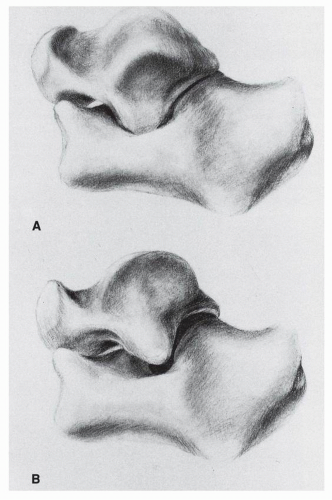 Figure 10.66 (A) Valgus of the heel: The calcaneus being held fixed, the talus moves in flexion-supination-adduction. The lateral process of the talus is low and strikes Gissane’s angle of the calcaneus. If the talus is held in neutral, then the calcaneus is in extension-pronation-abduction. (B) Varus of the heel: The calcaneus being held fixed, the talus moves in extension-pronation-abduction. The lateral process of the talus is high in position in the sinus tarsi. If the talus is held in neutral, then the calcaneus is in flexion-supination-adduction. |
degrees. With internal rotation force applied, calcaneotibial rotation increased from plantar flexion to neutral ankle position. With external rotation force applied, calcaneotibial external rotation from neutral to maximal dorsiflexion increased. Their conclusion was that “the ankle is less stable in plantarflexion when inversion and internal rotation forces are applied” and “the ankle was less stable in dorsiflexion when eversion and external rotational forces were applied.”
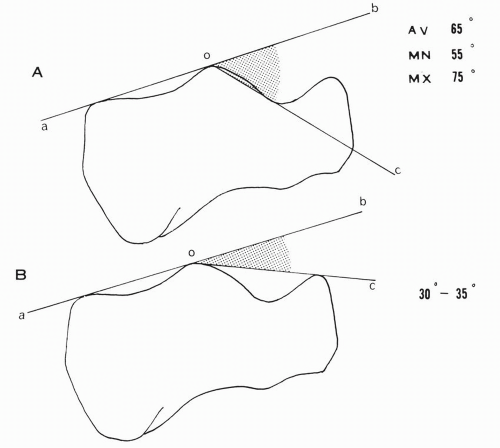 Figure 10.67 (A) Inclination angle of the posterior calcaneal surface. (B) Boehler’s angle. |
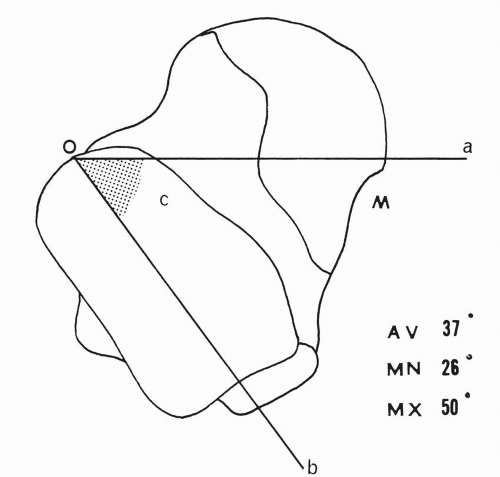 Figure 10.68 Declination angle of the posterior talar articular surface. |
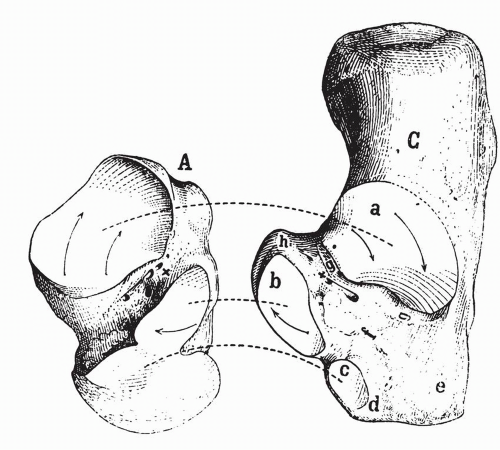 Figure 10.69 The rotational motion of the talus over the calcaneus. The arrows indicate the direction of rotation in a “tourniquet” fashion around the axis of rotation X located in the canalis tarsi. (A, talus; C, calcaneus; a, posterior calcaneal articular surface, cone shaped; b, sustentacular surface; c, anterior calcaneal surface.) (Farabeuf LH. Precis de Manuel Opératoire. Paris: Maisson; 1889:818.) |
of these functional discrepancies.32 Furthermore, the functional implication of the variable anatomic relationship between the calcaneofibular ligament and the lateral talocalcaneal ligament was investigated by Trouilloud and colleagues in 26 ankles.61 They divided their specimens into three types: A, B, and C. In type A (35%), a lateral talocalcaneal ligament blends with or reinforces intimately the calcaneofibular ligament and diverges from the latter at the talar or at the calcaneal insertion. In type B (23%), a distinct lateral talocalcaneal ligament is present just anterior to the calcaneofibular ligament. In type C (42%), the lateral talocalcaneal ligament is absent.
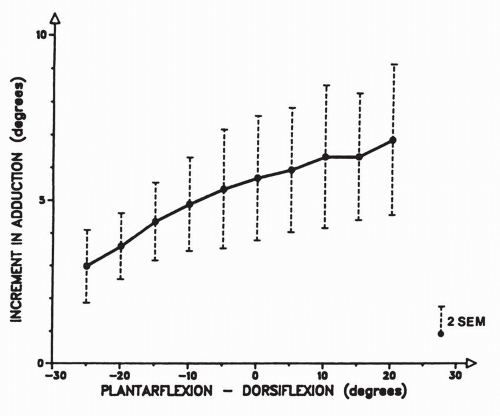 Figure 10.70 Mean increments of adduction (or supination) at the tibiotalocalcaneal joint complex after section of the calcaneofibular ligament in ten specimens. (Kjaersgaard-Andersen P, Wethelung J-O, Nielsen S. Lateral talocalcaneal instability following section of the calcaneo-fibular ligament: A kinesiologic study. Foot Ankle. 1987;7[6]:358.) |
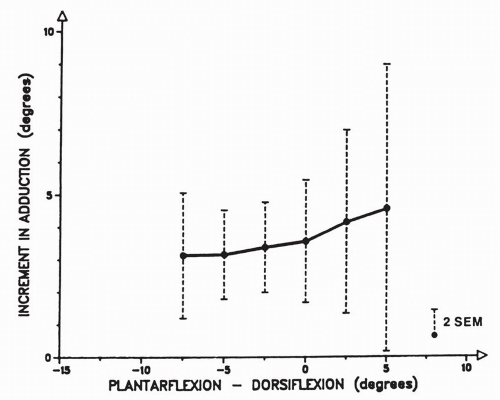 Figure 10.71 Mean increments of adduction (or supination) at the talocalcaneal joint after section of the calcaneofibular ligament in ten specimens. (Kjaersgaard-Andersen P, Wethelung J-O, Nielsen S. Lateral talocalcaneal instability following section of the calcaneo-fibular ligament: A kinesiologic study. Foot Ankle. 1987;7[6]:359.) |
of inversion assessment were used: manual and roentgenographic. Under inversion load with the calcaneofibular ligament intact the mean elongation of the cervical ligament was 0.58 mm ±0.33 mm by manual measurement and 0.46 mm ± 0.23 mm by x-ray measurement. With the calcaneofibular ligament transected, under inversion load, the elongation of the cervical ligament was 0.88 mm ±0.37 mm by manual measurement and 0.78 mm ±0.37 mm by x-ray measurement. With the transection of the calcaneofibular ligament, the inversion range of motion increased 7.5 degrees ± 2.75 degrees manually and 7.7 degrees ±2.95 degrees by x-ray measurement.
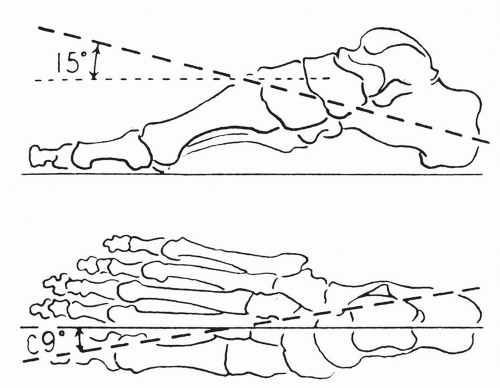 Figure 10.72 The longitudinal axis of the transverse tarsal joint projected in the sagittal and the horizontal planes of the foot. (Manter JT. Movements of the subtalar and transverse tarsal joints. Anat Rec. 1941;80:407.) |
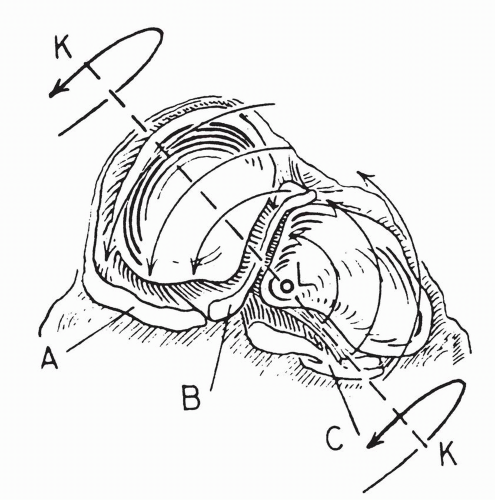 Figure 10.73 Posterior view of the right transverse tarsal joint shows the articular surfaces of the navicular and the cuboid. Light arrows indicate motion about a longitudinal axis L; heavy arrows indicate motion about an oblique axis KK. (A, plantar calcaneonavicular ligament; B, deep portion of the bifurcate ligament; C, long and short plantar ligaments.) (Manter JT. Movements of the subtalar and transverse tarsal joints. Anat Rec. 1941;80:404.) |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


