Chapter 10 From diagnosis to therapy
how to select points for treatment
INTRODUCTION
Once auricular diagnosis has been completed in all its aspects, it is time to start to treat. The therapist will need to make a selection of points which will be more or less complicated, according to his objective and the specific health problems presented by each patient. For example, to treat knee pain he will need to select one or more points in the area in which the knee is represented, be it French or Chinese. If instead he has identified a larger number of points and the syndrome is more complex, he will need to select those which are more effective and at the same time most suitable for a specific patient. Whatever the procedure he decides to adopt, there is an unwritten golden rule which says one should obtain the best result with the lowest number of points. This rule derives from body acupuncture which holds that a higher number of points does not produce better results but rather increases the risk of ‘hyperstimulation syndrome’ as defined by Pontinen,1 which can manifest by exacerbating pain in the 24–48 hours following an acupuncture session. This phenomenon is surely much less frequently observed in ear acupuncture which probably depends on the fact that ear stimulation is based on different reflexes than body acupuncture, or that auricular diagnosis correctly performed identifies the points which are strictly necessary to the patient. This selection therefore reduces the risk of stimulating a wrong or inappropriate auricular area.
Every physician will adopt his own strategy but in any case he will need to be fully acquainted with the patient’s condition and should be prepared, especially if symptoms are still insufficiently clear, to seek professional advice from other colleagues.
Another important factor in planning treatment is the evaluation of the patient’s compliance. Abbate2 wrote on this subject:
THE COMBINATION OF DIAGNOSTIC METHODS FOR SELECTING POINTS TO TREAT: A REVIEW OF THE LITERATURE
It is possible to produce a detailed review of the long sequence of books published on ear acupuncture since the publication of Paul Nogier’s historic treatise in French (1969) and in English (1972).3 A probably incomplete list of texts in English, French, German, Italian and Chinese is reported in Table 10.1.2–53 These different authors have detailed a variety of diagnostic methods, according to their skill, experience and will to describe a particular method. If we exclude the books featuring only one specific method we get an average of 2.2 methods per author. There are some major differences to note when comparing authors oriented more toward either the French or the Chinese schools of ear acupuncture. The former do not give primary importance to inspection and include the vascular autonomic signal (VAS) phenomenon among their diagnostic procedures. Physicians following the Chinese school, on the other hand, attribute major importance to inspection and do not follow any method related to the specific pulse diagnosis proposed by Nogier himself. However, all authors consider the contribution of the pressure pain test (PPT) and the electrical skin resistance test (ESRT) equally important in the detection and selection of auricular points to treat.
Table 10.1 Review of the diagnostic methods proposed by 52 textbooks on ear acupuncture/auriculotherapy
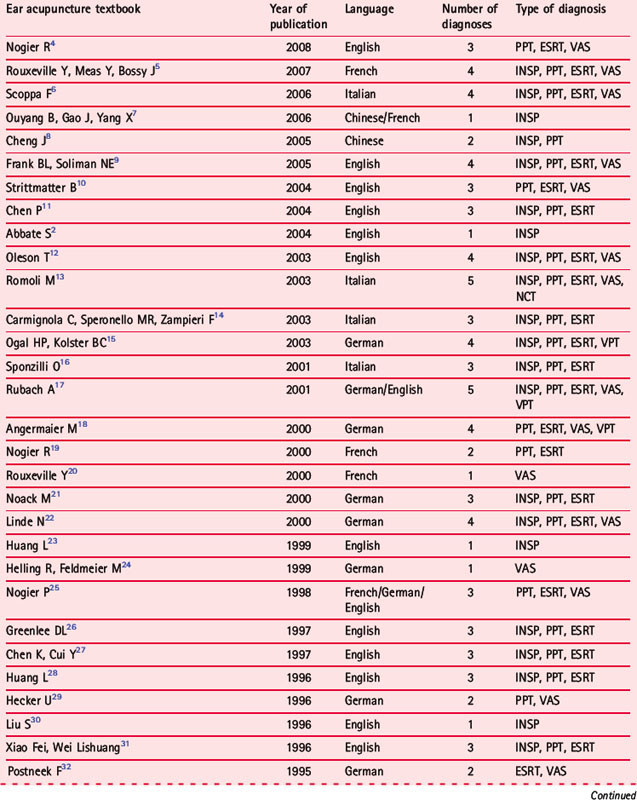
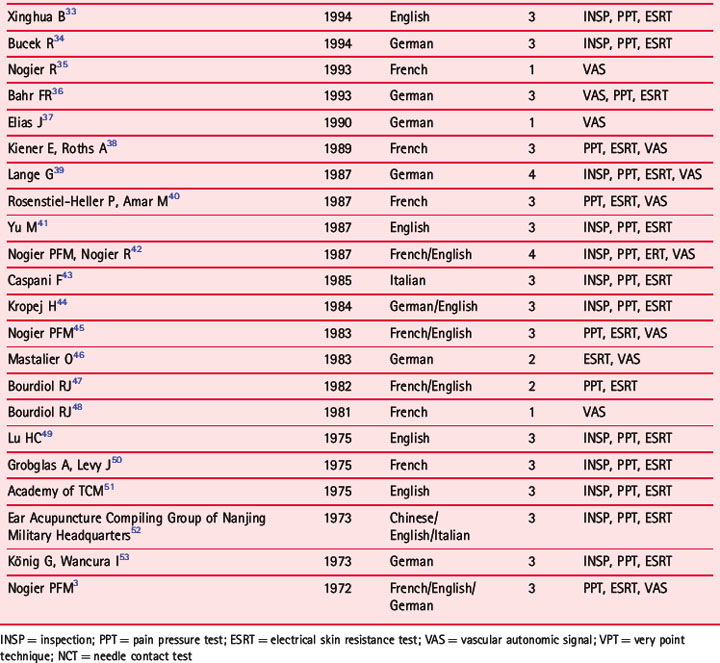
Some new methods possibly deserve attention, such as the ‘very point’ technique (VPT) proposed mainly by German authors, and the needle contact test (NCT) proposed by myself as a modification of Marcelli’s ‘active point test’ (see Ch. 8).
The reader will allow me a short digression on VPT, a diagnostic–therapeutic procedure which has some similarities to NCT. The technique was first proposed by Gleditsch54 for identifying body acupuncture points and other specific points such as those of mouth acupuncture. He used a short, fine injection needle for gently tapping out the skin area presumed to contain the acupuncture point to treat. The verum punctum or ‘very point’ corresponds to the center of the acupuncture point and when it is correctly identified it shows the following characteristics:
Angermaier18 and Rubach17 applied VPT to the auricle, tapping repeatedly or scraping the skin lightly with a very fine needle measuring 0.3 μm in diameter. This method does not traumatize the skin and any micro-bleeding of a point is part of the treatment itself and denotes local stagnation.
RESULTS OF A SURVEY CARRIED OUT ON 109 MEDICAL DOCTORS
A total of 136 colleagues, practicing members of the Federazione Italiana Società di Agopuntura (FISA), participated in a survey which I organized in 2002 for identifying the most important factors in the evaluation of adequate acupuncture treatment.55 The aim was to develop a possible scale to be used for systematic reviews on acupuncture.
The answers to the questionnaire are reported in Table 10.2.
Table 10.2 Diagnostic methods and selection of auricular points according to 109 physicians practicing ear acupuncture
| Auricular diagnosis | Yes | 67.0% |
| No | 17.4% | |
| Sometimes | 15.6% | |
| Total | 100% | |
| Diagnostic methods used (%) | Pain pressure test (PPT) | 35.3% |
| Inspection | 33.6% | |
| Needle contact test (NCT) | 16.4% | |
| Electrical skin resistance test (ESRT) | 11.8% | |
| Vascular autonomic signal (VAS) | 2.9% | |
| Total | 100% | |
| Combination of diagnostic methods (%) (in 81 physicians; 74.3% of the total) | Inspection + PPT | 30.9% |
| Inspection + PPT + NCT | 25.9% | |
| Inspection + PPT + ESRT | 9.9% | |
| Inspection + PPT + ESRT + NCT | 8.6% | |
| Inspection + ESRT | 3.7% | |
| PPT + NCT | 3.7% | |
| Other combinations | 17.3% | |
| Total | 100% | |
| Points selection according to TCM | Yes | 36.7% |
| No | 37.6% | |
| Sometimes | 25.7% | |
| Total | 100% | |
| Phases of Nogier | Yes | 8.2% |
| No | 78.0% | |
| Sometimes | 13.8% | |
| Total | 100% | |
| Formula acupuncture | Yes | 14.7% |
| No | 52.3% | |
| Sometimes | 33.0% | |
| Total | 100% |
WHICH STRATEGY SHOULD BE USED IN SELECTING POINTS?
1 Select first the areas which have been identified by more than one procedure
As reported in Chapter 9 (‘The topography of the identified auricular point/area’), the auricular somatotopic arrangement is essential for formulating a diagnostic hypothesis.
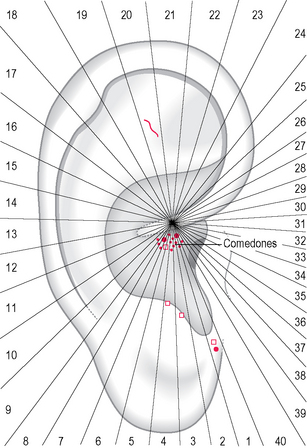
The practitioner who combines different methods may adopt his personal strategy in selecting the points to treat. For example, in the patient shown in Figure 10.1, who was affected by recurrent panic attacks, two areas were taken into consideration for treatment. The first, below the root of the helix, corresponding consistently to the Chinese esophagus area (CO2 shidao), was identified by inspection, PPT and ESRT. The second area, corresponding to Nogier’s fear area and the Chinese anterior ear lobe (LO4 chuiqian), was identified with PPT and ESRT. In this session the points detected on the antitragus with ESRT (possibly related to a past migraine) were not selected for treatment; neither was the Shen men area detected only by inspection (telangiectasia).
< div class='tao-gold-member'>

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


