Fracture Above Total Knee Arthroplasty: Femur
Supracondylar fractures above a total knee are more commonly associated with a poorly functioning arthroplasty. Stiffness and pain frequently predispose the patient to instability and a potentially traumatic event. A technically demanding, yet highly effective approach is to resolve both the failed arthroplasty and the fracture simultaneously. To treat the fracture alone merely returns the patient to the problematic preoperative status. Indeed, some problems such as a tight posterior cruciate ligament (PCL) will actually compromise healing because of persistent stress at the fracture site. The optimal approach is to resolve all these issues at one surgery. This requires extensive preparation for expected as well as unexpected techical difficulties.
Patient Presentation and Symptoms
- Acute: severe pain, hemarthrosis, often periarticular abrasions after minor trauma
- Chronic: mechanical periarticular pain, usually with a stiff joint and malunited or ununited supracondylar fracture
Indications
- Undisplaced fracture with failed arthroplasty
- Displaced fracture with or without successful arthroplasty
- Malunited fracture (usually in flexion, adduction, internal rotation)
Contraindications
- Excessive comminution
- Skin disruption
- Extensor tendon rupture
Physical Examination
- Hemarthrosis?
- Skin integrity?
- Extensor intact?
- Preoperative range of motion?
- Stiff or unstable total knee?
Diagnostic Tests
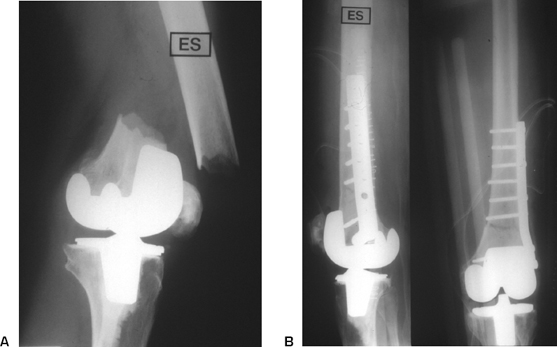
- Standard x-rays: multiple views to assess comminution and osteopenia (Fig. 46–1)
- Prefracture total knee films are helpful.
- “Normal knee” x-rays for prosthetic templating
Special Considerations
- Note degree of comminution and rarefaction of femoral bone
- Determine prefracture status of total knee arthroplasty (TKA)
- CR or PS TKA? Easiest to convert to PS knee at time of revision
Preoperative Planning and Timing of Surgery
- Operate within the first several days before fibrosis complicates surgery.
- Plan for intramedullary stems and supplemental fracture fixation such as plates and wires.
- Full revisional TKA equipment is needed as well as distal femoral replacement.
- Probable bone loss frequently requires allograft material.
- Be prepared to cement intramedullary stem.
- If the prefracture status of the knee was well-functioning then ORIF rather than revision may be optional (Fig. 46–2).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


