Foot fractures
Metatarsals and lisfranc injuries
INTRODUCTION
One often pictures elderly patients sustaining foot fractures falling from a standing height or less due to decreased visual, auditory or proprioceptive input, loss of strength, an inability to recognize and avoid hazardous situations, or for medical reasons such as syncope, cerebral vascular accidents, arrhythmias, or as a side effect of medications.1,2 and 3 However, the current elderly population is healthier, more mobile and much more active than previous generations. Although many exceed the national guidelines of moderate activity for at least 30 minutes per day,4 there are still sizeable numbers of patients who fail to meet these recommendations. Given these variable levels of activity and physiology, one can expect injuries to range from simple toe fractures to severe foot trauma.5,6 and 7
There are some problems however, when addressing elderly foot trauma. First, most studies are retrospective and discuss polytraumas or common injuries rather than specific problem areas. Secondly, bony and soft tissue injuries are often grouped together.8 Third, authors often describe the outcomes of all their patients rather than specifically targeting the elderly patient.9 Fourth, there is the difficulty in classifying fractures. Concerns about classifications include inter- and intraobserver reliability, ease of application, whether classifications are prognostic enough to guide treatment, and a consistent criticism that classifications are often too complex and serve better as a research tool. To improve dialog, historical and recently developed comprehensive classification systems will be discussed together. Lastly, it is difficult to decide how to classify someone as elderly, since there is no consensus concerning the age at which a patient is considered ‘elderly’.
Demetriades et al. recommended 70 years but were unable to draw any conclusions regarding the true impact of age.10 Classifying someone according to their physiology may be more important than simply classifying by age, but this too can be confusing. What we are certain of is that more people are living past 65 and that by 2040 some 21% of the US population will be 65 years and older.11
How then do we manage foot fractures in the elderly? Do we withhold certain treatments because they are too expensive? Studies have already shown that the cost of managing fractures and dislocations of the foot and ankle in the 2011 US Medicare population was approximately US$3.5 billion.12 Or do we withhold treatments due to expectations that the elderly will not do as well as nonelderly patients? This comes with the understanding that withholding treatment can produce avoidable complications, result in significant disabilities of the foot, create chronic pain conditions and lead to socioeconomic burdens on patients, their families and payer systems.
The decision driving treatment should be based primarily on the injury pattern and not solely on the patient’s age. If surgery is anticipated a discussion should include preoperative medical evaluations and the use of adjunctive fixation, cement and locking plate technology. Given the advances in techniques and implants, this chapter will hopefully provide a rational approach for the physician tasked with managing foot fractures in the elderly patient.
EPIDEMIOLOGY
Evaluating the incidence of elderly foot fractures is difficult because recent studies have poorly defined an elderly patient, have looked only at low-energy injuries or have looked only at fractures occurring in elderly women.13 In addition, foot trauma is often discussed presenting as a high- or low-energy injury rather than encompassing all foot injuries.5,6,14,15 and 16 Finally, the only injuries mentioning specific incidences, evaluations and treatment of foot fractures in the elderly are those involving the calcaneus.14,15 and 16
A recent study using data from the National Electronic Injury Surveillance System (NEISS) describing the anatomic site, disease category, age and circumstance of injury, analyzed all patients presenting to an emergency department with a lower extremity injury.9 Analysis of almost 120,000 reports from 1 January 2009 through 31 December 2009 revealed that the foot accounted for 15% of all lower extremity injuries with an additional 7% for toe injuries. In this study, the toe was the most common location (38%) for a fracture of the lower extremity with an additional 17% of lower extremity fractures located elsewhere in the foot. The authors also observed a correlation between increasing age and lower trunk fractures, allowing them to estimate the incidence of sustaining either a foot or toe fracture as 37 per 100,000/year (Table 43.1). Unfortunately, except for fractures of the toes, their findings did not segregate other anatomic locations of foot fractures nor did they specifically report the incidence of fractures in the elderly.
Currently, the best epidemiology on elderly foot fractures was presented in a 2-year review by Court-Brown et al.7 Data on all patients presenting to the Royal Infirmary of Edinburgh, Scotland, were collected from July 2007 to June 2008 and again from September 2010 to August 2011. Identifying fractures that occurred in patients 65 and older, the authors segregated the injuries into those involving the calcaneus, talus, midfoot, metatarsals and toe phalanges. The study identified metatarsal fractures as the most common foot injuries, with a rate of 67.6 (range 25.4–114.6) per 100,000/year. Toes (phalanges) were the next most frequent fractures, with a reported incidence of 8.5 (range 0–15.5) per 100,000/year. In the remaining three other locations, the incidences were 0.5 per 100,000/year (range 0–1.2) for talus fractures, 2.9 (range 0–5.1) for midfoot fractures and 4.7 (range 0–7.9) for calcaneus fractures (Table 43.1).
Table 43.1 Incidence of foot fractures
TALUS
The talus has no tendonous attachments and more than 60% of its surface is covered with articular cartilage. It is divided into a head, neck and body and articulates with the tibia, the fibular, the calcaneus and the navicular. The blood supply consists of an extraosseous and an intraosseous supply. The extraosseous supply arises from the dorsalis pedis, peroneal and posterior tibial arteries, with the latter two giving rise to the arteries to the tarsal sinus and the tarsal canal. The intraosseous supplies blood to the head, neck, the posterior talar tubercle and the medial talar body. The artery of the tarsal canal supplies most of the body while the artery of the dorsal pedis helps supply the head and neck.
Biomechanically, the talus links motion of the foot to the leg allowing gait to proceed from heel strike to toe lift. At the talocrural joint it allows dorsiflexion and plantar flexion. At the syndesmosis, during dorsiflexion, it produces external rotation of the fibula and internal rotation during plantar flexion. Through the subtalar joint, it contributes to flexion-abduction and extension-adduction of the hindfoot. It also contributes to pronation and supination as part of the transverse tarsal or Chopart’s joint at the midfoot. Therefore, malalignment can compromise motion of the ankle, subtalar and transverse tarsal joints.
Classification
Fractures are described involving the talar neck, body, head, lateral and posterior processes or as producing an osteochondral injury. Historically, talar neck fractures have been classified using Hawkins’ classification with the Canale–Kelly modification.17 Type I are nondisplaced fractures, type II are displaced fractures with subluxation of the subtalar joint, type III are displaced fractures with subluxation or dislocations of the subtalar and tibiotalar joints and type IV describes a type III fracture with an associated talonavicular dislocation.
Historical classifications for fractures of the body are not as commonly recognized and none has gained acceptance because classifications often combine both neck and body fractures. To differentiate these fractures, Inokuchi et al. stated that fracture lines exiting anterior to the lateral process were considered neck fractures and a talar body fracture if it existed posterior to the lateral process.18 Body fractures can also be described as osteochondral, coronal or sagittal shear, posterior tubercle, lateral process or crush fractures.
The Orthopaedic Trauma Association (OTA) compendium19 has classified all talus fractures into three simple groups: A, B and C. Group A describes fractures involving the lateral or posterior processes, the talar head or those producing an avulsion fracture. Group B divides talar neck fractures into three patterns: nondisplaced, displaced with subluxation of the subtalar joint or displaced with subluxation of both the subtalar and tibiotalar joints. The latter two are subdivided into noncomminuted, comminuted or those involving the talar head. Group C divides body fractures into dome fractures, those affecting the subtalar joint and those involving both the subtalar and tibiotalar joints. All three are also subdivided into noncomminuted and comminuted patterns.
Nonoperative treatment: talus
Nondisplaced fractures are uncommon injuries. Any fracture demonstrating more than 1 mm of displacement should be diagnosed as being displaced. Use of computed tomography (CT) scans and/or magnetic resonance imaging (MRI) confirms whether a patient can be treated nonoperatively.
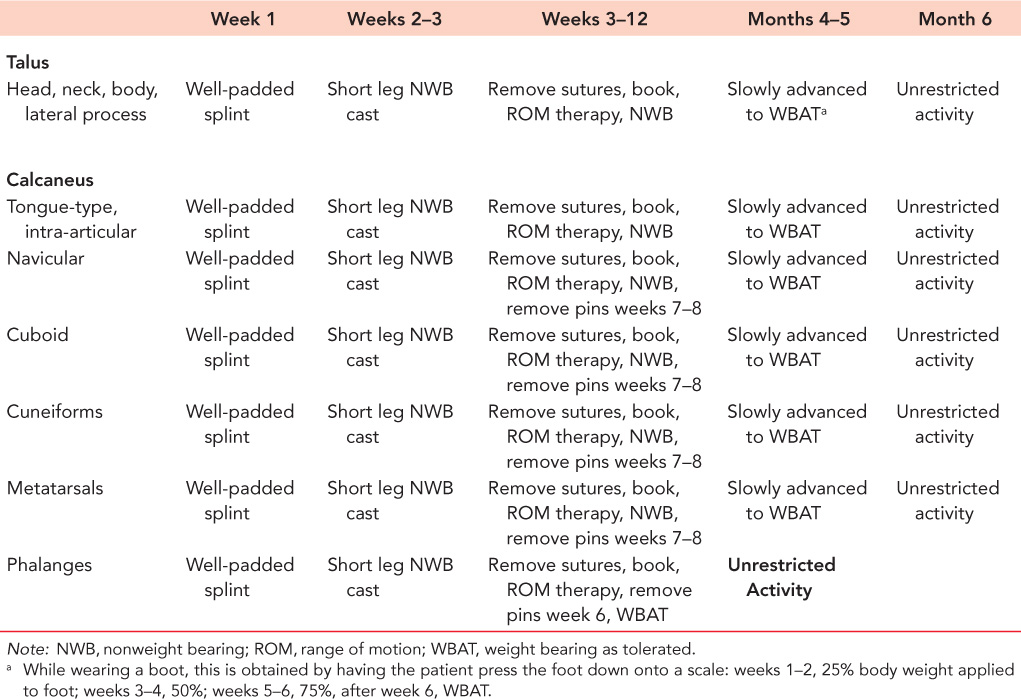
The authors’ preferred method of nonoperative treatment is a below knee nonweight-bearing cast for 6 weeks. The patient is X-rayed again in 2–3 weeks and after 6 weeks is placed into a removable boot and begins therapy. The patient is nonweight-bearing for the first 12 weeks and is then advanced to full weight bearing over the next 6 weeks.
Operative treatment: talar neck
Preoperative planning should include the use of small and minifragment instruments and implants, small headless screws and poly-L-lactic acid (PLLA) bioabsorbable pins.
Most fractures are managed through a dual incision approach. The anterolateral incision, or Böhler approach, begins between the bases of the third and fourth metatarsals and extends towards Chaput’s tubercle of the tibia. The superficial peroneal nerve is protected as it crosses the field (Figure 43.1) and the extensor retinaculum is divided exposing the extensor tendons. Retracting the tendons medially should allow one to see the tibial plafond, the dome, neck and head of the talus (Figure 43.2). The medial incision extends from the medial malleolus towards the tuberosity of the navicular, dorsal to the posterior tibial tendon (Figure 43.3). Working through both incisions allows visualization to determine whether an anatomic reduction has been obtained. Posterior and percutaneous approaches are rarely indicated because they do not allow for adequate visualization.
In fixation of closed fractures, there does not appear to be any difference whether they are treated before or after 6 hours.20 However, fracture dislocations should be reduced urgently in order to avoid necrosis of the underlying soft tissues. Unless there is comminution, compression techniques should be used to manage these injuries. Kirschner pins (K-wires) should only be used for provisional fixation. Definitive fixation is achieved using countersink screws placed retrograde, through the head, or antegrade, through the body, in order to prevent impingement during ankle or foot motion.
The goal is to place at least two screws across the fracture (Figure 43.4). On the lateral side of the talus, the authors’ preferred approach is a 2.7 or 3.5 mm cortical screw. This is placed either along the lateral border of the neck or through the lateral articular region of the talar head and is directed towards the posteromedial corner of the talar body. Medially, a retrograde 2.7 or 3.5 mm screw is placed through the inferomedial region of the talar head and directed towards the posterolateral corner of the talar body. Care should be taken to avoid screw penetration of the body posteriorly and the subtalar joint inferiorly.
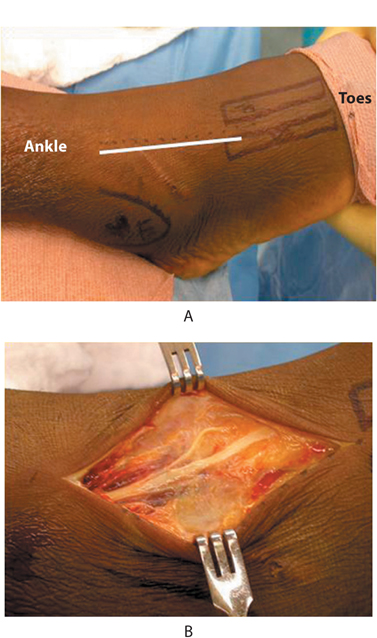
Figure 43.1 Anterolateral incision from the bases of the third to fourth metatarsals towards Chaput’s tubercle (a). Superficial peroneal nerve lies beneath the skin incision (b).
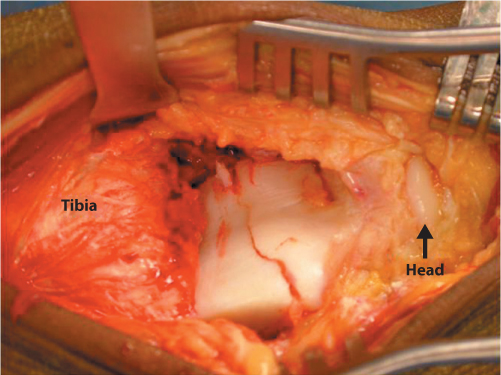
Figure 43.2 Deep dissection demonstrating the tibial plafond, dome, neck and head of the talus (black arrow).
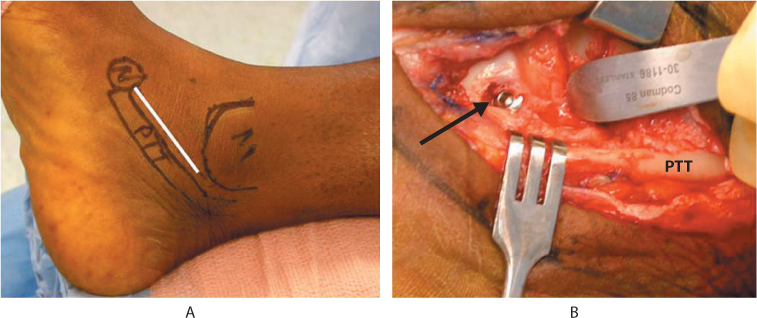
Figure 43.3 Approach from the medial malleolus to the navicular tuberosity (a). The deep dissection lies dorsal to the posterior tibial tendon (b). Note the countersunk screw through the head of the talus (arrow).
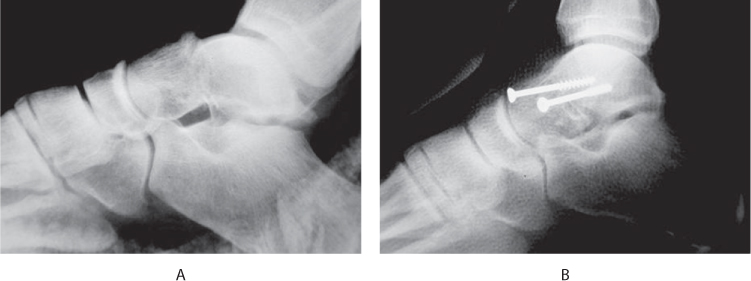
Figure 43.4 Pre- and postoperative lateral X-rays demonstrating a type II talar neck fracture (a,b).
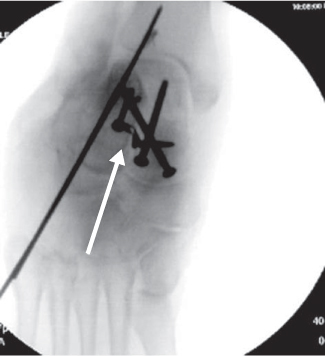
Figure 43.5 Canale view demonstrating a plate used to maintain talar neck length (arrow).
In the presence of comminution, compression technique should be avoided since it produces shortening of the neck and the medial column of the foot. Using transfixion (non-lag technique) screws or 2.4 or 2.0 mm minifragment plates is necessary in order to maintain length. If a plate is selected it can be safely placed along the lateral border of the neck, proximal to the head and distal to the lateral process, since this region is devoid of cartilage and will not interfere with any joint (Figure 43.5). It is also possible to place a very short plate along the medial border of the neck, proximal to the talar head and distal to the medial articular facet of the talus. Fluoroscopic views of the subtalar joint and neck can be used to gauge the reduction and length of the talus. For postoperative care see Table 43.2.
OUTCOMES AND COMPLICATIONS
Despite anatomic reduction, outcomes have demonstrated that significant functional impairment can be identified an average of 3 years post-fixation.21 Factors such as patient’s age, time to surgery and associated body fractures do not influence outcomes but comminution and dislocation or subluxation of the joint do.
Complications are divided into those occurring early and those occurring late. Early complications are due to malreduction of the fracture, often due to poor visualization of the fracture, medial compression of comminuted fractures, inadequate fixation of the fracture and early weight bearing. Late complications include delayed or nonunions, malunions, the development of osteonecrosis (avascular necrosis, AVN) and post-traumatic arthritis. Of these AVN has received the most attention. Historically, AVN has been reported to occur in 60–100% of all patients. However, recent studies report an incidence of 36–40%, regardless of the time to definitive fixation.20,21 Delayed unions or nonunions are relatively uncommon with a reported incidence of between 4% and 13%. They are often associated with a shortened talar neck and an adducted deformity of the forefoot, while malunions are often due to a missed fracture or loss of reduction. The most common late complication reported, however, is the development of post-traumatic arthritis, with studies reporting that 60–100% of patients will develop some arthritis in the ankle, subtalar or talonavicular joint.20,21
Table 43.2 Postoperative management of foot fractures
Operative treatment: talar body
Body fractures present as sagittal, coronal or horizontal patterns (Figure 43.6). To improve exposure, an osteotomy of the medial or lateral malleolus is often necessary. However, exposure to the lateral half of the talar body can also be facilitated using the Böhler approach. The medial incision begins proximal to the medial malleolus and extends distally (Figure 43.7). Once the medial malleolus is isolated, the authors’ preference is for a chevron osteotomy with the apex proximal to the articular surface (Figure 43.8). This osteotomy provides stability so that pre-drilling is not necessary. Starting with a small, oscillating saw, the osteotomy is completed using a flexible chisel. The medial malleolus is reflected distally, using the intact deltoid ligament as a hinge (Figure 43.9). If visualization is inadequate, a femoral distractor may be necessary to gain better access to the fracture.
Most fractures can be fixed using 2.7 or 3.5 mm screws, countersunk and placed perpendicular to the fracture line (Figure 43.10). If an adjacent osteochondral fragment is present, a PLLA pin or a small headless screw can also be used. For postoperative care see Table 43.2.
OUTCOMES AND COMPLICATIONS
Talar body fractures are significant injuries producing fair to poor outcomes. Open injuries and dislocations should be addressed emergently, however, neither the patient’s age nor time to definitive fixation affects outcome.21 What does affect outcomes is a malunion, AVN or post-traumatic arthritis. Malunions often result from inadequate visualization or poor reduction techniques, often after using closed, percutaneous methods (Figure 43.11). The development of AVN is seen with open fractures, those with significant comminution or associated talar neck fractures, with a reported incidence of 35–40%.22
The most common complication is the development of post-traumatic arthritis, often affecting the ankle and subtalar joints. Historically, the incidence has approached 90% for the ankle and 50% for the subtalar joint. However, recent literature has shown an incidence of 65% for ankle joints and 35% for the subtalar joint.22
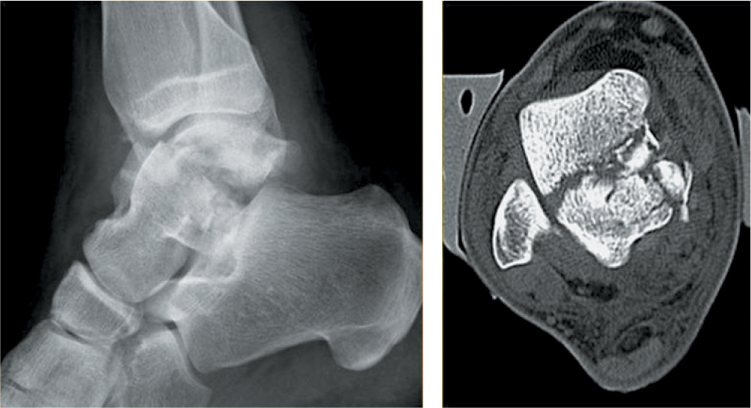
Figure 43.6 Lateral X-ray and an axial CT scan demonstrating a comminuted talar body fracture.

Figure 43.7 Medial approach to the ankle. The line indicates the position of the greater saphenous vein.
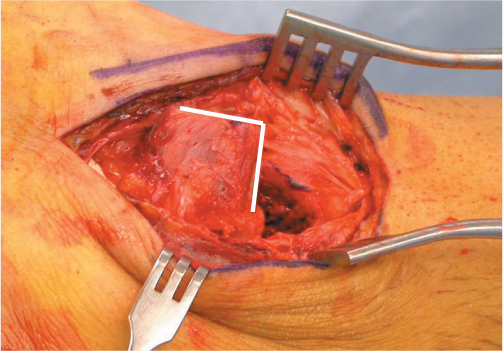
Figure 43.8 Chevron osteotomy has been completed using a flexible chisel.
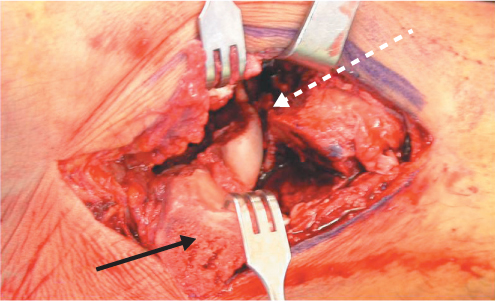
Figure 43.9 Deep dissection showing reflected medial malleolus (black arrow) and the talar body fracture (white dotted arrow). Visualization is improved with distraction.
Operative treatment: lateral process fractures
Lateral process fractures are often overlooked and account for 24% of all body fractures. They result from acute ankle dorsiflexion combined with inversion of the foot. A large, displaced fracture can produce chronic ankle instability (Figure 43.12).
The fracture is approached with an incision across the sinus tarsi (Figure 43.13). To improve visualization, distraction of the joint is often necessary. If the fragment is a single large piece, fixation is obtained using one or two 2.0 mm screws (Figure 43.14). If comminuted, a 2.4 or 2.0 locking plate is used to buttress the fracture. For postoperative care, see Table 43.2.
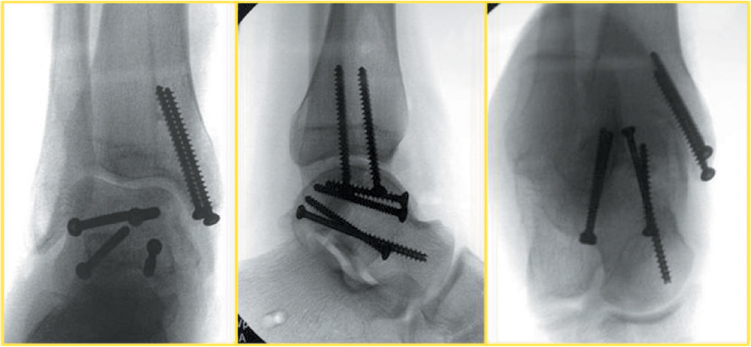
Figure 43.10 Anteroposterior (AP), lateral and Canale views demonstrating reduction of the talar body fracture and the osteotomy. Note the posterior screw below the articular surface.
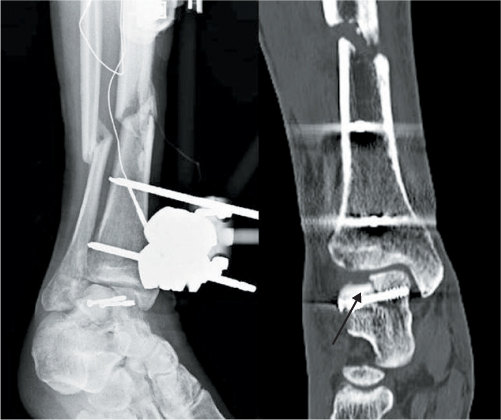
Figure 43.11 Oblique ankle X-ray and coronal CT scan demonstrating malreduction of a talar body, it was originally treated with two percutaneously placed screws (arrow).
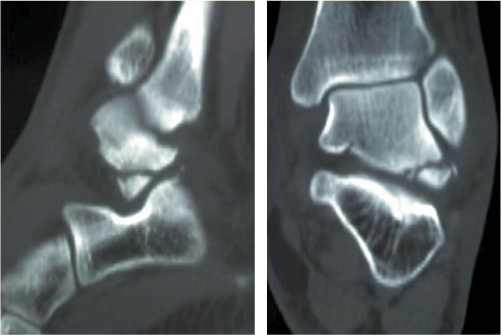
Figure 43.12 Sagittal and coronal CT scans demonstrating a lateral process fracture of the talus.

Figure 43.13 Surgical incision lies directly over the sinus tarsi and distal to the fibula.
OUTCOMES AND COMPLICATIONS
Outcomes and complications can be attributed to inadequately treated or missed injuries. The complications associated with this injury consist of chronic lateral ankle instability, nonunions, the development of subtalar arthrosis and potential impingement of the ankle along the talofibular joint.
Operative treatment: talar head fractures
Talar head fractures represent 5–10% of all talar fractures and present as a compression, from impaction with the navicular, or an oblique fracture, also identified as a shearing pattern, due to significant abduction/adduction of the foot.
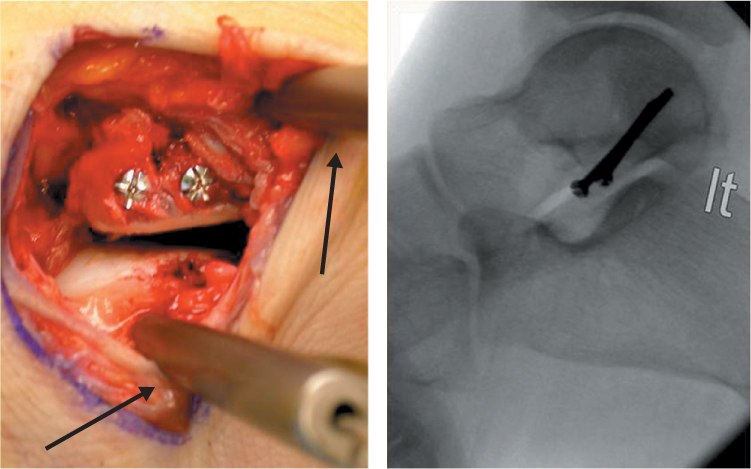
Figure 43.14 Fixation obtained using two 2 mm screws. Note pins used for joint distraction (arrows).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


