Fibrosarcoma and Desmoplastic Fibroma
FIBROSARCOMA
Fibrosarcoma in bone is a malignant tumor of spindle-shaped cells that does not produce osteoid material in either the primary lesion or the secondary deposits. Collagen production varies from abundant to none, tending to be less in the highly malignant examples. Fibrosarcoma may be so well differentiated that differentiating it from benign conditions such as fibrous dysplasia is difficult. The differentiation of fibrosarcoma from fibroblastic osteosarcoma and malignant fibrous histiocytoma may be somewhat arbitrary. Occasionally, matrix material is found only after a long search through many sections of the tumor that is predominantly fibroblastic, indicating that the distinction may be artificial.
After tumors that merely abutted on bone were excluded on the premise that they were probably of soft tissue origin, our series contained no distinct group of tumors that might logically be called “periosteal fibrosarcoma.” This manner of selection perhaps excludes some sarcomas of periosteal origin. From the gross pathologic features, it is apparent that most fibrosarcomas of bone arise in the medullary or the cortical regions, although a few undoubtedly begin in the periosteum.
“Secondary” fibrosarcoma accounted for just over 23% of the 286 fibrosarcomas in the Mayo Clinic files. (Table 13.1) Forty-eight occurred after radiation, four arose in giant cell tumors that had not been treated with radiation, seven occurred in Paget disease, and seven occurred in other conditions, including two ameloblastic fibromas, three bone infarcts, one fibrous dysplasia, and one odontogenic myxoma.
Three patients apparently had multicentric disease, but in only one patient was there histologic proof of involvement of more than one bone.
Some fibrosarcomas have a myxoid matrix. Such myxosarcoma-like foci may be prominent in some fibrosarcomas. Rarely, the entire tumor has an appearance that tempts one to designate it as a “myxosarcoma.” Transitional types between these and obvious fibrosarcomas make it reasonable to include such types with fibrosarcomas. Leiomyosarcoma has been described in several publications as occurring primarily in bone. Electron microscopic and immunoperoxidase studies seem to support this diagnosis.
INCIDENCE
The 286 fibrosarcomas comprised just over 4% of the total primary malignant bone tumors. Osteosarcoma is more than six times as common as fibrosarcoma in the Mayo Clinic files (Fig. 13.1).
SEX
There was a slight male predominance.
AGE
Fibrosarcoma does not show the marked propensity for patients in the second decade of life that osteosarcoma does. Instead, the tumors were more or less evenly distributed in patients in the second through seventh decades of life. Only one patient was younger than 5 years. The tendency of fibrosarcoma to occur among older persons as commonly as among younger ones is the major clinical difference between fibrosarcoma and osteosarcoma; 64 tumors occurred as late complications of preexisting conditions.
LOCALIZATION
The sites involved by fibrosarcoma do not differ remarkably from those involved by osteosarcoma. The region around the knee involving the distal femur and the proximal tibia was the most common location. Just over 50% of the tumors were located in the long bones, where the tumor is usually found in the metaphyseal region.
Several tumors that affected the maxillary antrum, including its bony walls, were excluded because they lacked evidence of an osseous origin. Three patients in the Mayo Clinic series had multifocal skeletal disease at presentation.
Several tumors that affected the maxillary antrum, including its bony walls, were excluded because they lacked evidence of an osseous origin. Three patients in the Mayo Clinic series had multifocal skeletal disease at presentation.
TABLE 13.1. Predisposing Conditions in 64 Patients with “Secondary Fibrosarcoma”* | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
SYMPTOMS
Fibrosarcoma produces the usual symptoms of malignant tumor in bone, namely, pain and swelling. Generally, these are of short duration. Patients whose fibrosarcomas arise secondarily give an appropriate history of the original condition and often had had radiation therapy many years before the malignant tumor appeared.
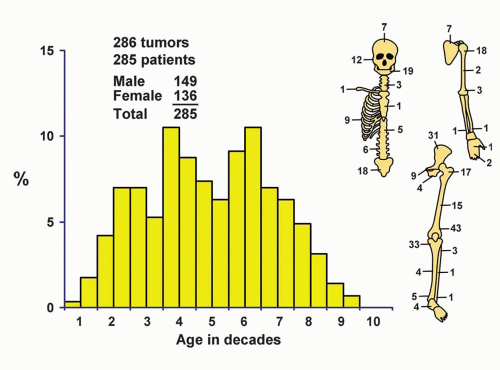 Figure 13.1. Distribution of fibrosarcomas according to age and sex of the patient and site of the lesion. |
PHYSICAL FINDINGS
Painful swelling in the region of the tumor is usually found unless the tumor is covered by a thick layer of uninvolved tissue. Spindle cell sarcoma, and even carcinomas with spindle-shaped cells, may metastasize to the skeleton and mimic primary fibrosarcoma, so evidence for such hidden lesions should be sought. Four patients with fibrosarcoma of bone had von Recklinghausen disease. Some of these sarcomas are pleomorphic and may be classified as malignant fibrous histiocytoma. None of the patients had evidence of neurofibromatous involvement of the bone.
The symptoms and physical examination are sometimes different in patients with fibrosarcoma secondarily to other conditions listed in Table 13.1. Fibrosarcomas that result from dedifferentiation of chondrosarcomas, as described in Chapter 6, are not included in these data.
RADIOGRAPHIC FEATURES
Fibrosarcomas of bone do not have radiographic features that differentiate them from lytic osteosarcomas. The lesions are purely lucent geographic areas of bone destruction and generally have features of malignancy, with cortical destruction and ill-defined borders. The radiographic appearance generally correlates with the histologic grade of the tumor. Well-differentiated tumors tend to be more sharply defined than poorly differentiated tumors. Taconis and van Rijssel found that the radiographic features of fibrosarcoma and malignant fibrous histiocytoma are essentially identical (Figs. 13.2, 13.3, 13.4 and 13.5).
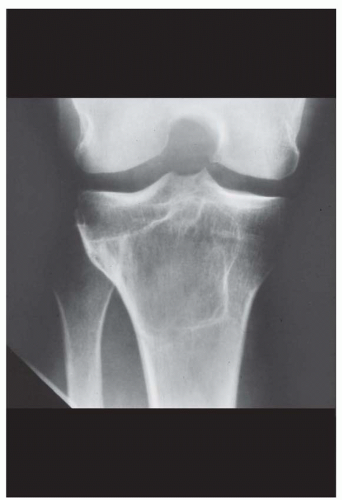 Figure 13.2. Grade 1 fibrosarcoma forming a well-demarcated, purely lytic lesion in the proximal tibia in a 47-year-old woman. The lesion has a sclerotic margin, suggesting a benign process. (Case provided by Dr. Alexander Templeton, Rush-Presbyterian-St. Luke’s Medical Center, Chicago, Illinois.) |
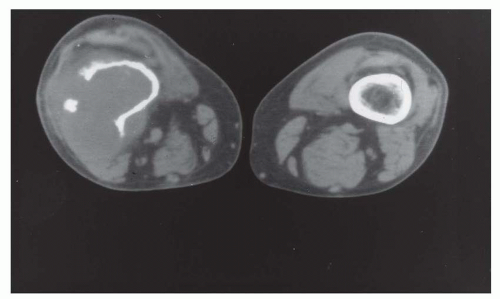 Figure 13.3. Computed tomogram of a grade 2 fibrosarcoma involving the distal femur in a 50-year-old man. The tumor has broken through the cortex to form a soft-tissue mass, suggesting a malignant process. |
 Figure 13.4. Grade 3 fibrosarcoma arising in the ilium in a 59-year-old woman. The tumor was resected without any neoadjuvant chemotherapy. There was no matrix production in the resected specimen. |
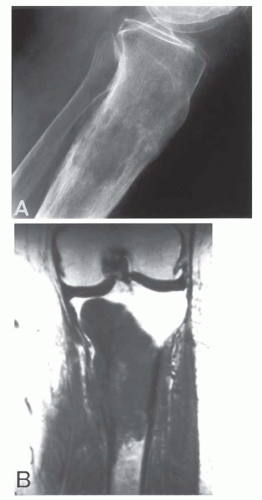 Figure 13.5. Leiomyosarcoma involving the proximal tibia in a 70-year-old woman. There was no primary tumor elsewhere. A: The radiographic appearance is that of a malignant tumor but is otherwise nonspecific. B: Magnetic resonance imaging shows destruction of cortex with involvement of soft tissue. (B, From Young, C. L., Wold, L. E., McLeod, R. A., and Sim, F. H.: Primary Leiomyosarcoma of Bone. Orthopedics, 11:615-618, 1988. By permission of publisher.) |
GROSS PATHOLOGIC FEATURES
The gross appearance of fibrosarcoma also varies according to the histologic grade. Low-grade sarcomas tend to be firm and fibrous and may have a whorled appearance. High-grade sarcomas tend to be soft and fleshy. The tumor may have a glistening appearance because of the presence of a myxoid matrix. The bone is invaded in an irregular fashion and the margins may be indistinct. At presentation, almost all the fibrosarcomas of central origin have broken through the cortex and have a large or small extraosseous component. The gross specimen may show evidence of a preexisting condition such as Paget disease or an infarct (Figs. 13.6




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
