Angiosarcoma and Hemangiopericytoma
Malignant vasoformative tumors comprise one-half of 1% of malignant neoplasms in this series. These lesions have varied from such highly anaplastic ones that recognizing them as spindle cell sarcoma with vasoformative capability is difficult, and sometimes is manifested only in part of the tumor, to well-differentiated neoplasms that are questionably malignant. The terminology used in the discussion of malignant endothelial tumors has been quite confusing. The terms hemangiosarcoma, angiosarcoma, hemangioendothelioma, and hemangioendothelial sarcoma have all been used either as synonyms or to denote separate pathologic entities. Some authors use the term angiosarcoma to denote the very malignant vascular tumors and the term hemangioendothelioma to denote low-grade malignant neoplasms. Hemangioendothelial sarcoma, although descriptive, is cumbersome. In the latest edition of the World Health Organization Classification of bone and soft tissues, the accepted term is angiosarcoma.
Vascular spindle cell sarcomas that are not of provable endothelial origin and metastatic carcinoma are differential diagnostic problems. Metastatic carcinoma, especially renal cell carcinoma to bone, may be very vascular, and its aggregates of plump cells mimic those of some angiosarcomas.
Multifocality, especially in a limited portion of the skeleton (e.g., in one extremity), may occur in as many as one-third of patients. Hemangiopericytoma of bone is extremely rare. There were only 15 examples in the Mayo Clinic files. When a diagnosis of hemangiopericytoma of bone is considered, it is imperative to rule out a primary lesion elsewhere, such as in the meninges.
ANGIOSARCOMA
INCIDENCE
The 109 cases in the Mayo Clinic files comprised just over 1.5% of malignant tumors of bone (Fig. 23.1).
SEX
There is a slight male predominance, with approximately 59% of the patients being male.
AGE
Angiosarcoma tends to affect young and older adults. Only three patients were younger than 10 years. The distribution is more or less even from the second through the seventh decades of life.
LOCALIZATION
Angiosarcoma may affect any portion of the skeleton. There is a tendency toward the axial skeleton, with approximately one-third of the lesions involving the spine and pelvic bones. Fifteen lesions involved the small bones of the hands and feet. Thirty-five of the 109 patients had multifocal disease. In two of these cases, there were multiple lesions in one bone. By far, the most common manifestation of multifocality was in the same topographic area, such as involvement of multiple bones of one extremity. This pattern occurred in 20 patients. However, in 13 patients, the tumor involved different areas of the skeleton.
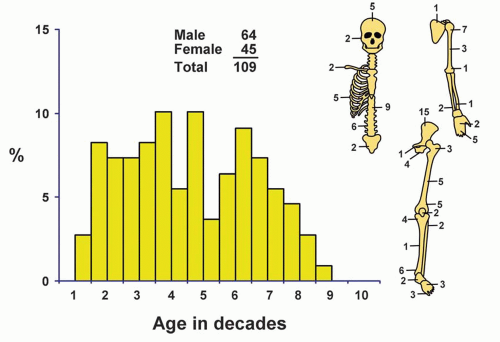 Figure 23.1. Distribution of angiosarcomas according to age and sex of the patient and site of the lesion. |
SYMPTOMS
There were no specific symptoms, although pain was usual.
PHYSICAL FINDINGS
There were no specific physical findings, but tenderness was sometimes elicited locally.
RADIOGRAPHIC FEATURES
The majority of angiosarcomas produced a purely osteolytic lesion. Occasionally, a tumor has a mixture of lysis and sclerosis. Some low-grade tumors showed well-marginated areas of lysis, with or without a sclerotic rim. However, most tended to be poorly marginated, with the lesion gradually fading into the surrounding bone. Periosteal reaction is unusual and usually associated with the production of a soft-tissue mass. A soft-tissue mass is more commonly associated with a higher grade of malignancy. The occurrence of multiple lytic lesions, especially in contiguous bones, strongly suggests a diagnosis of angiosarcoma (Figs. 23.2, 23.3, 23.4, 23.5, 23.6, 23.7 and 23.8).
GROSS PATHOLOGIC FEATURES
The lesional tissue is typically bloody, suggesting its primary vascular nature. The tumors are usually soft. Although the presence of a soft, bright red lesion, especially when multifocal, may suggest the diagnosis of angiosarcoma, there are no gross pathognomonic features (Figs. 23.7 & 23.9, 23.10 and 23.11).
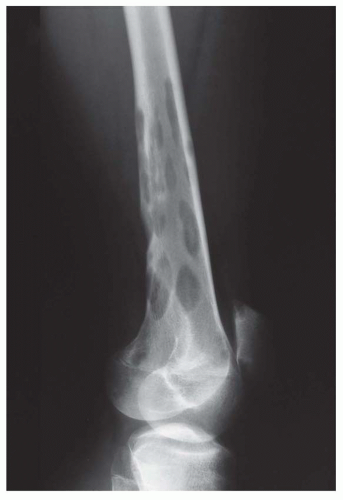 Figure 23.2. Plain radiograph of the distal femur in a 14-year-old boy with multicentric grade 1 hemangioendothelioma. There are multiple well-defined lytic defects in the bone. Some of these defects have destroyed the cortex. Other bones in the legs were also involved. |
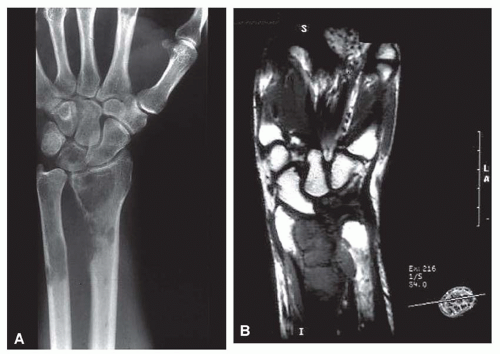 Figure 23.3. Anteroposterior radiograph (A) and coronal T1-weighted magnetic resonance image (B) of the distal forearm and wrist show multiple osteolytic lesions involving the distal radius, ulna, and lunate bones. The lesion in the radius shows cortical destruction with an associated soft-tissue mass. The imaging features of the lesions are nonspecific, but the multiplicity of lesions clustered in a geographic region such as the distal extremity suggest that the diagnosis is low-grade angiosarcoma. |
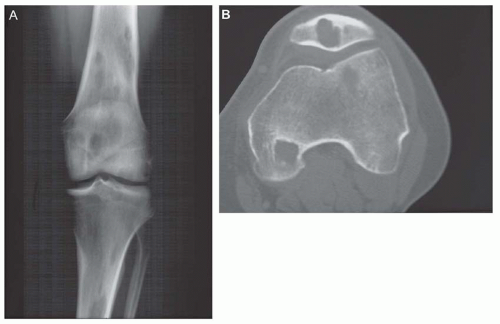 Figure 23.4. A: Multicentric grade 1 angiosarcoma involving multiple bones in the region of the knee in a 47-year-old man. B: Computed tomogram shows multiple lesions. |
 Figure 23.5. Anteroposterior radiograph (A) and coronal T1-weighted magnetic resonance image (B) of the right foot show severe osteoporosis associated with multicentric angiosarcoma forming destructive osteolytic lesions involving the third through fifth metatarsals. All the lesions have malignant aggressive features, with cortical destruction and associated malignant periosteal new bone formation. Panel B shows that the lesion of the forth metatarsal is associated with a pathologic fracture. |
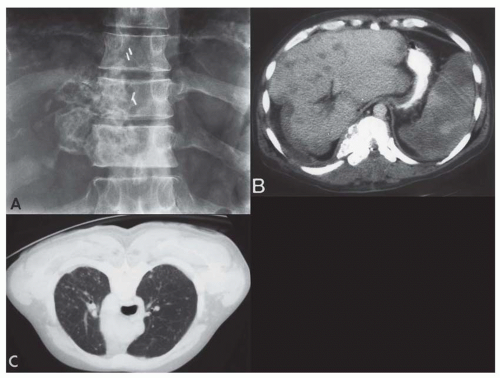 Figure 23.6. Epithelioid hemangioendothelioma in a 42-year-old man. A: Radiograph shows a partly sclerotic lesion of a vertebral body. B: Computed tomography shows multiple foci of involvement of the liver in addition to the sclerosing lesion of the vertebral body. C: Computed tomography of the lung shows diffuse involvement of the pulmonary parenchyma with epithelioid hemangioendothelioma. The patient died of disease within 1 year. |
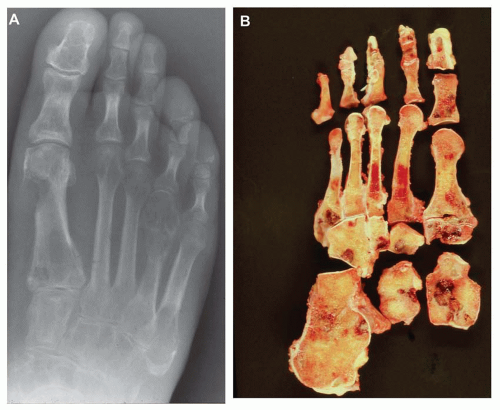 Figure 23.7. A: Grade 1 hemangioendothelioma involving multiple small bones of the foot. Some of the lesions have destroyed the cortex and extended into soft tissue. B: Gross specimen in a case similar to that in A. Multiple dark red areas correspond to the vascular neoplasm. There is no fleshy tumor-like material. |
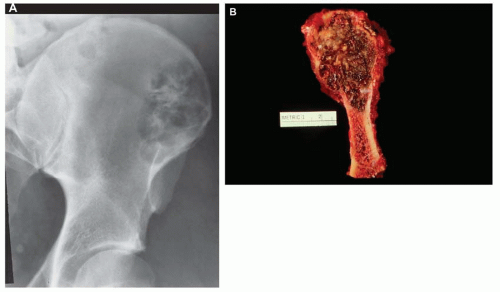 Figure 23.8. Epithelioid hemangioendothelioma involving the ilium in a young man. A: The lesion is lucent but has areas of sclerosis. The margins are well defined and lobulated. B: Corresponding gross specimen with a lobulated, dark red neoplasm. |
HISTOPATHOLOGIC FEATURES
To qualify as angiosarcoma, the lesion had to have tumor cells that formed vascular spaces. However, there was much variation in the quality and quantity of the vascular spaces formed. In low-grade lesions, the tumors tended to have well-formed vascular spaces lined by tumor cells showing slight atypia. In grade 2 lesions, the vasoformation was still quite obvious. The cells lining the vascular spaces tended to have a more cuboidal appearance and cytologic atypia. Mitotic figures were also more common. Grade 3 lesions tended to show either sharply circumscribed spaces lined with obviously atypical cells or spindling malignant tumors in which the vascular spaces were less obvious. The cells tended to be loosely arranged and some showed clefting containing red blood cells. The vascular spaces tended to anastomose with one another, especially in the lower- and medium-grade tumors. The spaces in high-grade tumors may be separated, although desmoplastic reaction is unusual (Figs. 23.12




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
