Benign Chondroblastoma
Benign chondroblastoma is a neoplasm of bone that has been separated from giant cell tumors because of a chondroid matrix. The basic proliferating cells of the neoplasm may be remarkably similar to those of a true giant cell tumor, but these cells can produce foci of chondroid matrix, so it is logical to include chondroblastoma among the tumors of cartilaginous origin. Because of the unusual cytologic characteristics of the mononuclear cells, a reticulohistiocytic origin has been suggested for chondroblastoma. Electron microscopic and immunoperoxidase studies have supported a cartilaginous derivation for this neoplasm.
Although some of the features of this neoplasm were recognized earlier, it was not until 1942 that the term benign chondroblastoma was introduced and distinctive clinicopathologic features were delineated. The cellular zones of these tumors ordinarily contain at least a few mitotic figures. These, coupled with chondroid zones, have led to the erroneous diagnosis of malignant giant cell tumor. In fact, one of the main reasons for recognizing this entity is that clinically it is relatively nonaggressive and readily curable, even more so than ordinary giant cell tumor.
Most studies have indicated a close relationship between benign chondroblastoma and chondromyxoid fibroma. Although some authors have suggested the possibility of a malignant chondroblastoma, there are no such examples in the Mayo Clinic files. Some chondroblastomas have metastasized as benign tumors and some have produced huge, occasionally lethal, local recurrences. The term “aggressive” has been used for these lesions. Cytologically, however, these aggressive and metastasizing chondroblastomas are indistinguishable from the more common benign lesions; hence, the terms aggressive and “malignant” do not appear to be reasonable. These terms may be used for describing clinical features but not pathologic entities. Some osteosarcomas have cytologic features remarkably similar to those of chondroblastoma. Hence, these rare tumors and clear cell chondrosarcomas have to be considered when neoplasms behave aggressively.
INCIDENCE
The Mayo Clinic series contains 147 examples of chondroblastoma, which constitutes 4.79% of all benign lesions and 1.45% of all neoplasms of bone (Fig. 4.1). Chondroblastoma is approximately one-fifth as common as a giant cell tumor.
SEX
In the Mayo Clinic series, just over 60% of the patients with benign chondroblastomas were male. In a larger series, including consultation cases, published from Mayo Clinic, the male-to-female ratio was 2:1.
AGE
More than 60% of all patients were in the second decade of life. The youngest patient was 8 years old and the oldest, 60.
LOCALIZATION
Chondroblastomas are typically centered in an epiphysis (Fig. 4.1). Although they occur most often in the end of a major tubular bone, they can appear in any center of ossification, such as the greater trochanter. The region of the knee accounted for 34% of all the tumors; the proximal tibia was involved slightly more often than the distal femur. Chondroblastoma involved the patella in four patients, accounting for 50% of all benign tumors in that bone and 28.6% of all tumors. The proximal humerus was the single most common site, accounting for just less than 20% of all sites. The proximal femur was involved in 20 patients; of these chondroblastomas, six involved the greater trochanter. Seventeen patients were older than
40 years; five of them had involvement of the temporal bone (Kurt and associates also found that patients with chondroblastoma of the skull bones tended to be older than patients with chondroblastoma of the long bones). One typical chondroblastoma was centered in the metaphysis. A diagnosis of chondroblastoma-like osteosarcoma has to be ruled out when this tumor occurs in an atypical site. There has been one documented example of two chondroblastomas occurring in one patient. There are no such examples in the Mayo Clinic files.
40 years; five of them had involvement of the temporal bone (Kurt and associates also found that patients with chondroblastoma of the skull bones tended to be older than patients with chondroblastoma of the long bones). One typical chondroblastoma was centered in the metaphysis. A diagnosis of chondroblastoma-like osteosarcoma has to be ruled out when this tumor occurs in an atypical site. There has been one documented example of two chondroblastomas occurring in one patient. There are no such examples in the Mayo Clinic files.
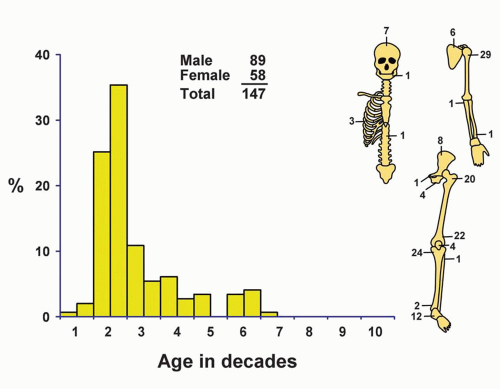 Figure 4.1. Distribution of chondroblastomas according to age and sex of the patient and site of the lesion. |
SYMPTOMS
Local pain is the most important symptom of benign chondroblastoma and affects most patients. Turcotte and coauthors reported that 86% of patients had pain. The average duration of symptoms was 20 months (range, 5 weeks to 16 years). The other symptoms reported were swelling, a limp, and joint stiffness. Lesions in the temporal bone were associated with progressive loss of hearing and earache.
PHYSICAL FINDINGS
About 45% of patients have a tender area on palpation. The less common findings are decreased range of motion in a nearby joint, muscular atrophy, a palpable mass, and soft-tissue swelling.
RADIOGRAPHIC FEATURES
Characteristically, benign chondroblastoma appears as a central area of rarefaction. A typical feature of chondroblastoma is its location within the involved bone. In the series reported on by Kurt and associates, 37% of the lesions that involved the long bones were entirely within the epiphysis, and 60% involved the epiphysis and extended through the epiphyseal plate into the adjacent metaphysis. Thus, 97% of chondroblastomas of long bones were either entirely epiphyseal or had an epiphyseal component. The finding of a lesion involving both sides of an open epiphyseal plate is practically diagnostic of chondroblastoma. Only one chondroblastoma recorded in the Mayo Clinic files was entirely metaphyseal. Most chondroblastomas involve the medullary cavity, although rarely they may appear to involve the cortex. There were no examples of chondroblastoma presenting as a surface or soft-tissue lesion (Figs. 4.2, 4.3, 4.4, 4.5, 4.6 and 4.7).
Approximately one-fourth of the lesions in long bones in the report by Kurt and associates involved an apophysis, either the greater trochanter of the femur or the greater tuberosity of the humerus.
Chondroblastomas tend to form a round or an oval defect in the involved bone. Nearly half the tumors
have a surrounding thin sclerotic rim. Two-thirds of chondroblastomas do not show mineralization. Computed tomographic scans may show mineral not visualized on plain radiographs. Approximately three-fourths of chondroblastomas involve the adjacent cortex. Periosteal new bone formation is seen rarely (Figs. 4.2, 4.3, 4.4 and 4.5).
have a surrounding thin sclerotic rim. Two-thirds of chondroblastomas do not show mineralization. Computed tomographic scans may show mineral not visualized on plain radiographs. Approximately three-fourths of chondroblastomas involve the adjacent cortex. Periosteal new bone formation is seen rarely (Figs. 4.2, 4.3, 4.4 and 4.5).
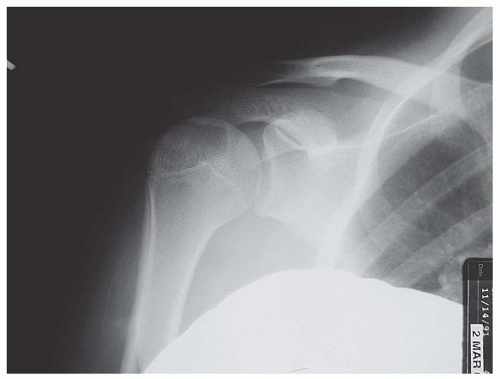 Figure 4.2. Chondroblastoma involving the proximal humerus in a 14-year-old girl. Anteroposterior plain film shows a lucent lesion in the epiphysis, with associated periosteal reaction. |
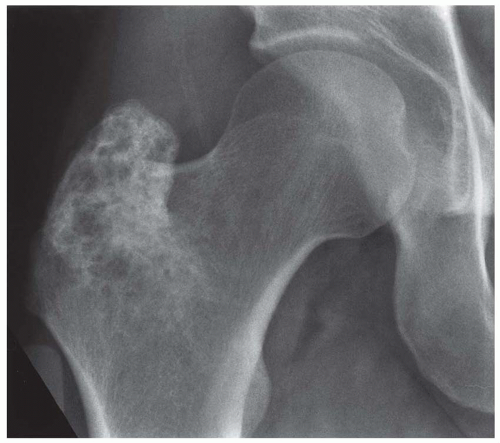 Figure 4.3. Mineralized chondroblastoma involving an apophysis—the greatest trochanter of the femur—in a 28-year-old man (Case provided by Dr. David H. Houn, St. Bernard’s Regional Medical Center, Jonesboro, Arkansas). |
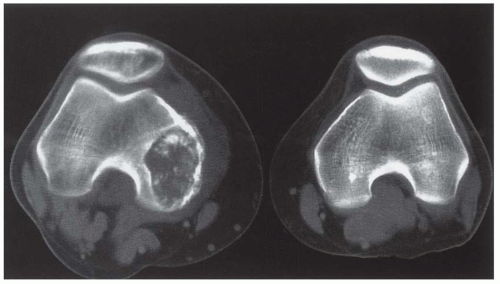 Figure 4.4. Computed tomographic appearance of chondroblastoma in a 19-year-old man. The lesion is well marginated and contains mineral (Case provided by Dr. J. Adolph, St. Paul’s Hospital, Saskatchewan, Canada). |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


