Malignant Fibrous Histiocytoma
Numerous reports of malignant fibrous histiocytoma of bone have been reported. A typical neoplasm is one that shows fibrogenic differentiation, often in a “storiform” pattern, and has other areas of cells with nuclei that are similar but appear to be histiocytic. The nuclei are often indented, the cytoplasm is usually abundant and may be slightly foamy, the nucleoli are often large, and multinucleated malignant giant cells are usually a prominent feature.
Many osteosarcomas, fibrosarcomas, and dedifferentiated chondrosarcomas contain areas that resemble what is regarded as malignant fibrous histiocytoma. When sections of all parts of a malignant tumor fit the histologic pattern, the designation of malignant fibrous histiocytoma seems appropriate. The finding of even minute foci of definite chondroid or osteoid matrix excludes the tumor from the group of malignant fibrous histiocytomas.
In 1977, a series of 35 examples of malignant fibrous histiocytoma were reported from Mayo Clinic. These were collected from a review of 158 fibrosarcomas and 962 osteosarcomas in the files at that time. Seventeen of the malignant fibrous histiocytomas had been previously quoted as “fibrosarcoma” and 18 as “osteosarcoma.” Since then, tumors have been coded separately as malignant fibrous histiocytoma when appropriate. There are 98 examples of these tumors, compared with 1,952 osteosarcomas and 285 fibrosarcomas.
Several electron microscopy studies have indicated the similarity between these tumors and the malignant fibrous histiocytoma primary in the soft tissues. The tumors are apparently composed of cells with the capability of differentiating along fibroblastic and histiocytic lines.
Although most authors agree that malignant fibrous histiocytoma is a clinicopathologic entity, its true histogenesis is still controversial. Some studies have suggested that these tumors are of histiocytic derivation, whereas others have suggested that they are fibroblastic. It is possible that the entity of malignant fibrous histiocytoma encompasses a variety of very pleomorphic sarcomas of bone and soft tissue.
INCIDENCE
Only 98 examples of malignant fibrous histiocytoma were found among the total of 7,098 primary malignant tumors (Fig. 15.1).
SEX
There was only a slight male predominance, with 57 males and 41 females. In a report of the largest series of malignant fibrous histiocytomas of bone to date, Huvos and coauthors found that males constituted approximately 58% of the population.
AGE
Nearly any age may be affected; only one patient was younger than 10 years. This was a 6-year-old girl with a tumor of the sacrum. The age distribution is more uniform than that of osteosarcoma and similar to that of fibrosarcoma.
LOCALIZATION
Many different bones were affected, but the long bones were the site in 62 cases, with the region of the knee being the most common location. Only one patient presented with a multicentric process; this tumor has been reviewed several times and it does not appear to be an example of lymphoma simulating malignant fibrous histiocytoma.
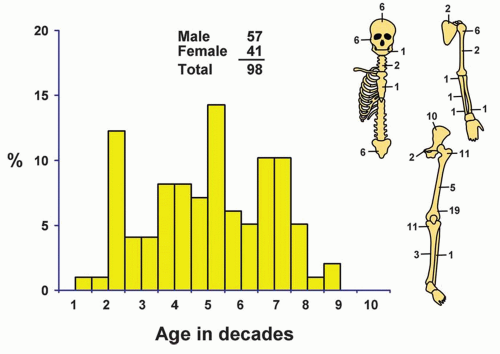 Figure 15.1. Distribution of malignant fibrous histiocytomas according to age and sex of the patient and site of the lesion. |
SYMPTOMS
As with other varieties of bone tumor, pain and swelling were the most frequent symptoms. One patient had symptoms for only 1 week, but most had symptoms for 6 months or more. Three of the tumors complicated Paget disease of bone, and 12 developed in bones that had been affected by previous radiation therapy. Two malignant fibrous histiocytomas arose in association with bone infarct. One arose at the site of a previous total hip arthroplasty. Troop and coauthors and Haag and Adler also have reported a case each of malignant fibrous histiocytoma at the site of a previous total hip replacement. Hence, 24.1% of all malignant fibrous histiocytomas have to be considered secondary. Huvos and coauthors reported that 28% of the malignant fibrous histiocytomas of bone were considered secondary.
PHYSICAL FINDINGS
Pain or swelling or both were noted as a consequence of the local lesion.
RADIOGRAPHIC FEATURES
The most common appearance is that of a purely lytic destructive lesion. Cortical destruction is almost always present and usually extensive. Cortical breakthrough with an associated soft-tissue mass is common. The features are those of an aggressive malignant tumor. The differential diagnosis includes osteosarcoma in younger patients and fibrosarcoma, lymphoma, metastasis, and myeloma in older patients (Figs. 15.2, 15.3 and 15.4).
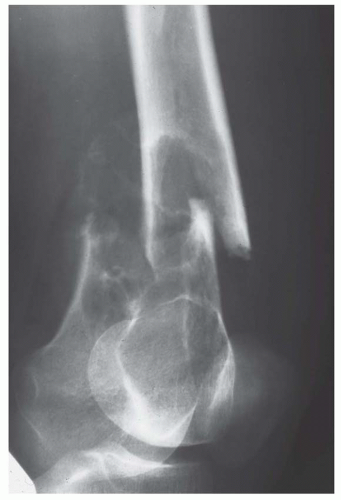 Figure 15.2. Malignant fibrous histiocytoma associated with a pathologic fracture in the distal femur in a young woman. The lesion is purely lytic, although there is some sclerotic reaction in the soft-tissue extension. |
 Figure 15.3. Anteroposterior radiograph of a malignant fibrous histiocytoma forming a destructive mass at the site of a previous arthroplasty in the femur in a 72-year-old man. He had knee replacement surgery 9 years before this tumor was detected. |
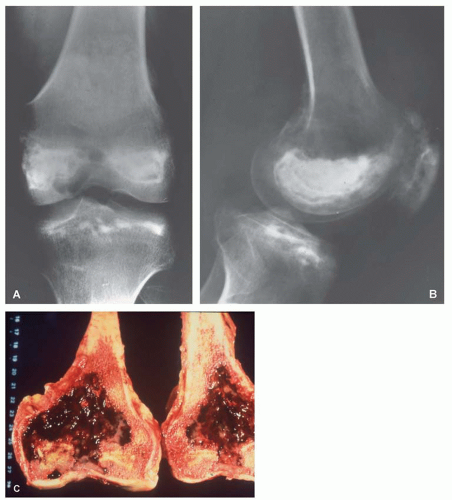 Figure 15.4. Anteroposterior (A) and lateral (B) radiographs of malignant fibrous histiocytoma associated with an infarct involving the distal femur in a 61-year-old man. Pancreatitis had developed approximately 40 years earlier. Infarcts are seen in the femur and the tibia. The gross specimen (C) shows infarct in the distal portion of the bone. The tumor is dark red and has destroyed the cortex. |
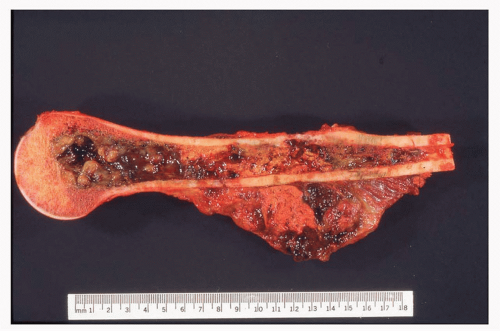 Figure 15.5. Malignant fibrous histiocytoma in a 22-year-old man. This tumor forms a partially hemorrhagic mass that extensively involves the proximal and mid humerus and is associated with extension into soft tissue. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


