Experimental Models of Femoroacetabular Impingement
Timo M. Ecker
Marc Puls
Klaus A. Siebenrock
Experimental Models of Femoroacetabular Impingement
Diagnosing Femoroacetabular Impingement
Although primary idiopathic osteoarthritis of the hip joint is a rare phenomenon (1,2,3), it has become clear that distinct structural deformities of the femur and acetabulum lead to a gradual deterioration and development of secondary arthritis of the hip joint (4). Femoroacetabular impingement (FAI) has been identified as one of the conditions associated with an increased incidence of arthritis in patients under 60 years of age (5,6). Ever since FAI has been recognized as a prearthrotic deformity, intense research has been absolved to investigate etiology and pathophysiology of the underlying disease. Different subtypes of FAI have been described, depending on the location of predominant pathology (7,8,9). Pincer Impingement is associated with acetabular pathology. Deformity presents in terms of profound or protruding, as well as partially or globally retroverted acetabula (10). Cam-type impingement is eponymous for femoral pathology. The femoral head–neck junction in patients with cam-type impingement is not spherical due to a variety of conditions, hence reducing femoral head–neck offset (11,12,13,14,15). Both subtypes coexist frequently, resulting in mixed-type impingement.
During hip joint range of motion (ROM) these deformities lead to recurrent impingement between the acetabular rim and the femoral head–neck junction, resulting in a characteristic damage pattern at the acetabular cartilage and labrum (6). In isolated pincer-type impingement, where the femoral head–neck junction is configured normally, the damage occurs initially at the acetabular labrum. The repetitive contact with the femoral bone leads to cystic degeneration and thinning of the labrum. In addition, bony apposition at the osseous acetabular rim can be found. The protruding acetabular rim furthermore crams into the femoral head–neck junction, leading to indentation lines and herniation pits. The concomitant levering causes damage in the posteroinferior portion (6) of the acetabular cartilage because of levering forces grinding the femoral head into this part of the joint and leading to a contrecoup lesion. In cam-type impingement, the damage is caused by the incongruity of the articulating joint couples. In isolated cam-type impingement, the aspherical head–neck junction forces itself into the normally configured and hence comparably small acetabulum. Whereas pincer-type impingement leads to direct stress load at the labrum, the impingement bump in cam-type impingement undermines the acetabular labrum and detaches the adjacent acetabular cartilage at the site of load distribution. True labral damage occurs later in cam-type impingement, with progressive damage of the acetabular cartilage and decentering of the femoral head.
The clinical diagnosis is secured by certain clinical and radiographical tests. Specific clinical tests include the anterior and posterior impingement tests, the FABER (flexion, abduction, external rotation) test, and the log roll test, where collision between head–neck junction and acetabular rim is provoked, to elicit pain (16). The radiographic diagnosis is based predominantly upon conventional x-rays. Hence, the primary standard imaging study for assessment of a patient with the clinical diagnosis of FAI is a set of conventional radiographs consisting of an anteroposterior (AP) view and axial cross table view of the affected hip joint (17,18). Additional views to assess the joint in more detail include the false profile of Lequesne to evaluate anterior acetabular coverage (19), as well as frog-leg lateral and the modified Dunn/Rippstein projection to assess the morphology of the femoral head–neck junction and proximal femur (20). A variety of parameters which are indicative for FAI and associated with development of osteoarthritis of the hip joint can be assessed on plain x-rays (21).
Apart from conventional radiography, the modality of choice to investigate the hip joint in more detail is magnetic resonance imaging (MRI) in terms of an arthro-MRI. Here, the use of specific contrast agents and special radial sequences spanning a 360-degree view of the hip joint, offer enhanced possibilities for assessment of labral injuries of cartilage changes secondary to FAI (22,23,24,25).
Rationale for Creating Models of Femoroacetabular Impingement
Despite the amount of knowledge gathered, questions remain regarding the natural behavior of the disease and
the exact associated pathomorphologic changes inflicted to the cartilage of the hip joint. The employment of models for improved understanding of this disease is of major importance to improve future diagnostic and treatment strategies.
the exact associated pathomorphologic changes inflicted to the cartilage of the hip joint. The employment of models for improved understanding of this disease is of major importance to improve future diagnostic and treatment strategies.
First, experimental models can aid in comprehending assumptions regarding characteristic patterns of damage caused to the joint by the distinct deformities. Observations drawn from the clinical routine can be confirmed by reconstructing, simulating, and investigating models resembling the situation encountered in vivo.
Second, experimental models can be used to investigate affected hip joints in more detail and thus confirm and refine the diagnosis. FAI is not a static but rather dynamic disease and becomes apparent during movement of the hip joint, when the proximal femur and acetabulum collide. Even though the above described diagnostic methods are applied routinely, none of these tools allow for assessing this dynamic component of the disease. The point in time when impingement occurs during ROM, as well as the exact location and geographic extent of abnormal femoral and acetabular contact stresses can only be estimated and is not grasped by these examinations. Third, the stress load distribution and the resulting physical deformity throughout the joint during femoral and acetabular collision cannot be assessed with conventional methods. To investigate these parameters, different models of FAI have been created.
Current Models
An Animal Model for Experimentally Induced Cam Impingement in the Sheep Hip
Rationale for This Model
As described above, in early studies investigating osteoarthritis of the hip, femoral deformity had already been suspected to cause acetabular cartilage degradation. However, until the propagation and refinement of the FAI concept (7) and the introduction of a safe surgical method for dislocating the hip joint without compromising the blood supply of the femoral head (8,26), there was no possibility to accurately assess the actual damage of the acetabular cartilage. The above described cartilage lesions in cam impingement are typically visible in the anterosuperior quadrant of the acetabulum, where the maximum stress forces during flexion and internal rotation are assumed (6). In addition, patients with a nonspherical femoral head predominantly present with a “tongue-like” extension of the capital cartilage onto the anterosuperior portion of the neck with distinct discoloration and degenerative signs within the nonspherical portion as opposed to normal appearing cartilage in the central portion (27). To verify the assumption that these observed changes to the joint are indeed associated with the cam-type deformity an animal model was created. Although general animal models for investigation of osteoarthritis are unspecific and lead to a global degradation of the joint (28), one of the challenges of this study was to develop an animal model that would merely simulate cam impingement with its typical behavior and damage pattern. With such a model it was deemed possible to obtain improved insight into not only macromorphologic changes, but also alterations at the histologic level. Secondarily, this knowledge could be used to investigate correlation to cartilage degeneration in clinical and MRI findings, which might aid in estimating effectiveness of different treatment modalities and potential future treatment options.
Methods
Finding the Adequate Animal
In previous research, the femoral morphology of several species had been compared with the human femur (29). Although morphology of the normal human femur is more alike in certain primate or canine species, it was found that the femoral head–neck junction in sheep closely resembles the aspheric human head–neck junction encountered in cam-type impingement (Fig. 39.1). Furthermore, the configuration of a sheep acetabulum, although more shallow, is very similar to the human one, including an acetabular labrum, horseshoe-shaped cartilage lamination, and a central fossa. Apart from the morphologic similarities, sheep have become a standard model for investigation of biologic response during healing, as well as analysis of posttraumatic mechanical alterations. Fields of research include among others, evaluation of effectiveness of cartilage repair (30) and meniscal healing in the knee joint (31). Also, sheep do not have a known predisposition for development of hip joint pathology, and their pain susceptibility is significantly lower than it is in canine experimental animals. This allows for an early mobilization and rapid weight bearing after surgery.
Artificial Creation of Femoroacetabular Impingement
After sheep had been chosen as the animal of choice, the next step was to evaluate how the underlying “pistol-grip” morphology of the sheep’s hip joint could be utilized to cause a collision conflict with the acetabulum. Hence, in a first experimental series, 10 cadaver hip specimen of 3- to 4-year-old Swiss mountain sheep were examined. Sheep in this age have the advantage, that the proximal femoral growth plate has already ossified, but the hip joint is still at a young age, reducing the likelihood of arthritis. The above mentioned morphologic properties were confirmed in all specimen. To create impingement, it became obvious that the aspherical femoral head–neck junction had to be approximated to the acetabular rim. Abduction of the leg did rotate the femoral head medially toward the centre of the acetabulum and created a visible impingement conflict during the end range of hip flexion with the posterosuperior portion of the acetabulum. Hence, to achieve this effect, an extracapsular medial closed wedge osteotomy at the intertrochanteric level was performed and consecutively fixed with a lateral plate (Fig. 39.2). Wedge angles of 10, 15, and 30 degrees were evaluated. As expected, increasing wedge angles led to a decrease of ROM in regard to flexion and internal rotation. Although in normal stance the cam deformity remained laterally to the acetabular rim, it jammed into the posterosuperior portion of the acetabulum, once hip flexion was increased to 70 to 90 degrees. With the sheep’s four-legged stance and a resting position of 90 degrees in the hip joint, the posterosuperior portion of the acetabulum, which represents the most lateral position, could be exposed to cam-type impingement. After these initial experiments, wedge angles between 10 and 30 degrees were deemed sufficient for artificial impingement creation.
Pilot Study
After construction of an experimental model, the next step was to investigate, whether the ex-perimentally created deformity would lead to the expected
structural and biologic changes within the hip joint. Therefore, veterinary IRB approval was obtained and eight Swiss alpine sheep with an age range of 3 to 4 years received the above described closed wedge osteotomy unilaterally, with a random left-to-right distribution leaving the contralateral hip as a control group. To investigate the adequate wedge angle, two groups were formed with four sheep receiving a 15-degree wedge osteotomy and four other sheep receiving a 30-degree osteotomy. To approximate an appropriate time for development of cartilage changes, ambulatory periods until sacrifice were 16, 20, 24, and 28 weeks.
structural and biologic changes within the hip joint. Therefore, veterinary IRB approval was obtained and eight Swiss alpine sheep with an age range of 3 to 4 years received the above described closed wedge osteotomy unilaterally, with a random left-to-right distribution leaving the contralateral hip as a control group. To investigate the adequate wedge angle, two groups were formed with four sheep receiving a 15-degree wedge osteotomy and four other sheep receiving a 30-degree osteotomy. To approximate an appropriate time for development of cartilage changes, ambulatory periods until sacrifice were 16, 20, 24, and 28 weeks.
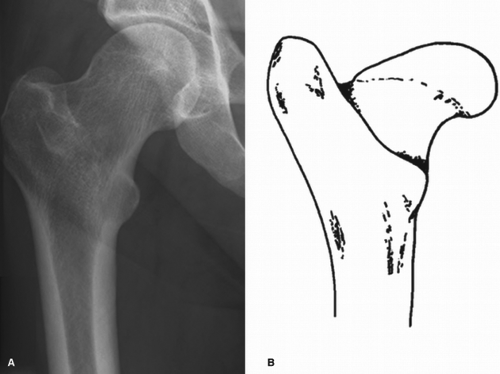 Figure 39.1. A comparison between an anteroposterior radiograph of a human femur with a cam-type deformity (A) and a drawing of a typical proximal femur of a sheep (B) is depicted. The similarity between the pistol grip deformity of the human femur and the physiologic aspheric head–neck junction in sheep can be seen. |
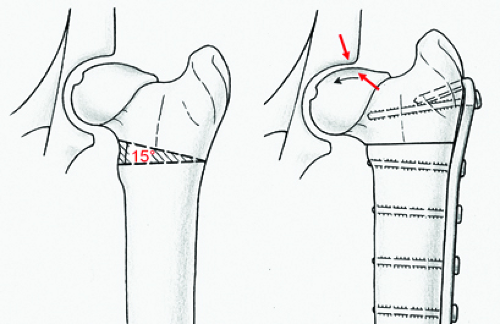 Figure 39.2. The closed wedge osteotomy at the proximal femur of the sheep is shown. At the intratrochanteric level a 15-degree wedge is resected medially. The closed wedge osteotomy is stabilized laterally using a double-hook plate (Synthes Vet, Synthes AG, Switzerland). This leads to a greater varus orientation of the proximal femur. Consequently, the aspheric femoral head–neck junction is approximated to the acetabular rim. Although physiologically no impingement occurs between femur and acetabulum due to the sheep’s four-legged stance, this experimental morphologic alteration now causes impingement at the posterosuperior portion of the joint (red arrows). This is similar to the cam-type pathomechanism at the anterosuperior portion of the hip joint in humans. |
The results of this pilot study confirmed the experimental model to be appropriate. Seven of the eight sheep showed focal degeneration at the predicted posterosuperior portion of the acetabulum, including labral tears with adjacent cartilage delamination. One sheep with a 15-degree osteotomy did not show visible signs of lesions after the shortest postoperative follow-up of 16 weeks. Histologically, however, there were changes in the hyaline cartilage in the region mentioned above of the acetabulum in all sheep. This was controlled by also examining the contralateral hip joints, where neither macroscopic, nor histologic changes of the cartilage could be noted.
Also noted was subluxation of the treated hip joint in one of the sheep with a 30-degree osteotomy.
Concluding from these results, regarding the osteotomy angle, the 15-degree wedge appeared to be sufficient, to avoid possible subluxation of the hip joint, while at the same time producing impingement. Regarding the follow-up period, since no macroscopic evidence of general cartilage degeneration throughout the entire joint but only focal damage were visible, the follow-up period was extended.
Main Study
After the experimental model had been established the actual main study was performed. For this study 16 Swiss mountain sheep with an age range of 3 to
4 years were chosen and a 15-degree varus osteotomy at the proximal femur was performed with a random side distribution, resulting in eight left and eight right femora.
4 years were chosen and a 15-degree varus osteotomy at the proximal femur was performed with a random side distribution, resulting in eight left and eight right femora.
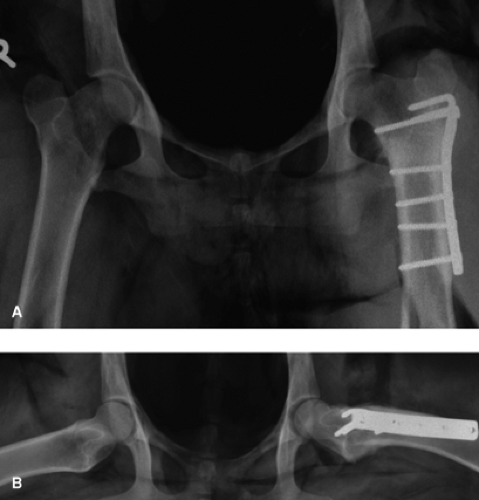 Figure 39.3. Postoperatively, anteroposterior (A) and lateral (B) x-rays of the operated hip joint were obtained to confirm concentric position of the head and implant positioning. |
Surgical Procedure and Follow-Up
Sheep were positioned in the lateral position; the previously clipped area was prepped and draped in sterile manner. After a curved incision above the greater trochanter, the exposure of the proximal femur was established by partial release of the vastus lateralis and intermedius muscle. After preparation of the lesser trochanter, the extra-articular osteotomy was performed, creating a 15-degree medial wedge. The osteotomy was closed medially and stabilized laterally, using a double hook plate (Synthes Vet, Synthes AG, Switzerland), as used for intertrochanteric osteotomies in dogs (Fig. 39.2). Interfragmentary compression was achieved by eccentric drilling for the cortical bone screws. After plate fixation, the muscles were reattached and layer-wise wound closure was performed. Immediately postoperatively, an AP and lateral radiograph of the operated hip joint were obtained (Fig. 39.3). Supplied with adequate pain medication the sheep were transferred to their box and a suspension device for restriction of weight bearing was applied immediately. The animals were recovered in slings and were supervised until full consciousness. The suspension device was worn for 4 weeks, to allow for healing of the osteotomy. After that, the animals were kept in small stalls for another 4 weeks and subsequently were allowed to roam freely. The 16 sheep were divided into four groups of four sheep each. A different time of follow-up was assigned to each group, being 14, 22, 30, and 38 weeks of follow-up. After that the animals were sacrificed and immediately after, another AP and lateral pelvis x-ray of the operated hip joint was obtained.
Evaluated Parameters
Joint Partition
Dissection of the joint was performed and the capsule was freed from surrounding muscle and soft tissue. After the capsulotomy, presence and color of joint effusion was noted. Subsequently, the femoral head was dislocated from the acetabulum. For the upcoming macroscopic and histologic examinations, the acetabulum and the femoral head were mapped in a standardized manner and for simplification of orientation considered all right hips. The reference area for the femoral head was the frontal aspect of the femoral head and neck as limited by an AP plane through the head–neck axis. Furthermore, a central weight-bearing area was distinguished from a lateral nonweight-bearing area (Fig. 39.4). The acetabulum was defined in a clock-like manner as usually done for evaluation in human hip joints: zone A representing the posterosuperior area (7 to 9 o’clock), zone B representing the craniomedial area (12 to 2 o’clock), and zone C anteroinferior area (4 to 6 o’clock) (Fig. 39.4).
Macroscopic Analysis
To assess the macroscopic changes, the labrum, adjacent cartilage, general cartilage, and the synovial lining of the joint were examined and photodocumented. Damage to the cartilage and labrum were classified according to the recommendations of Beck et al. (6).
Histologic Analysis
Histologic specimen of the acetabulum were obtained from the above described topographic regions of the acetabulum. Care was taken, that the longitudinal specimen included all regions of the acetabulum (fossa, hyaline cartilage with subchondral bone, and acetabular rim including labrum). The blocks were then cut
in halves longitudinally, to be available for two different analyses. For the first analysis, hyaline cartilage exhibiting the macroscopically most obvious damage was dissected with a scalpel blade and subsequently deep frozen for further immunohistochemical analysis. For the second analysis, the full-thickness specimen were fixed in 4% Paraforma ldhyde for 24 to 28 hours. The femoral head specimen were obtained by division of the frontal plane in halves and were then processed similarly.
in halves longitudinally, to be available for two different analyses. For the first analysis, hyaline cartilage exhibiting the macroscopically most obvious damage was dissected with a scalpel blade and subsequently deep frozen for further immunohistochemical analysis. For the second analysis, the full-thickness specimen were fixed in 4% Paraforma ldhyde for 24 to 28 hours. The femoral head specimen were obtained by division of the frontal plane in halves and were then processed similarly.
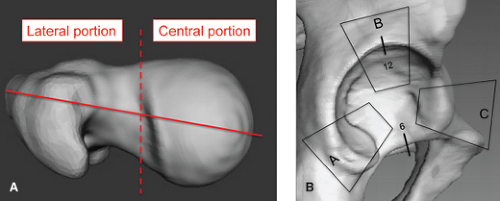 Figure 39.4. The femur (A) and acetabulum (B) were mapped to allocate findings during macroscopic and microscopic analyses to reproducible portions of the joint. The reference area for the femur was located anteriorly to a longitudinal transection plane through the head and neck. It was furthermore divided into a central, weight-bearing portion and a lateral nonweight-bearing portion. The acetabulum was defined in a clock-like manner, with the 6 o’clock position representing the teardrop. Zone A represents the dorsolateral area (7 to 9 o’clock), zone B represents the craniomedial area (12 to 2 o’clock), and zone C the anteromedial area (4 to 6 o’clock). |
Table 39.1 Distribution of Acetabular Cartilage Damage Divided by the Acetabular Zonesa | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
After fixation in Paraformaldehyde, the specimen were treated through a graded series of ethanol, defatted in xylene and subsequently embedded in an acrylic resin. The bone blocks were polymerized in Teflon forms at 32 degrees in a water bath. After embedding in HistoDur, the nondecalcified specimen were then cut with a microtome, resulting in 30- to 40-μm cuts for the acetabular specimen and 5-μm cuts for the femoral specimen. All specimen were consecutively stained using Toluidine blue. Afterward, the specimen were microscopically assessed for cartilage fraying or clefting, cell proliferation and cluster formation, tidemark alterations or duplication and proteoglycan depletion analysis was performed. To classify cartilage damage, the Mankin classification is applied (32,33). Both macroscopic and histologic analyses were performed for all operated and nonoperated control hip joints.
Results
The surgical procedure and the postoperative follow-up period occurred uneventful in all 16 cases according to the assigned duration of follow-up. The immediate post operative and postsacrifice x-rays documented correct implant positioning and excluded subluxation of the hip joints or secondary dislocation of the osteotomy.
Macroscopic Findings
Acetabulum
The most apparent cartilage damage occurred in zone A, the posterosuperior aspect of the joint. The cartilage damage was noted in 15 of 16 operated hip joints and ranged from malacia over combinations of malacia and debonding to cleavage lesions of the cartilage (Table 39.1). Labral damage occurred in this zone in 14 of 16 operated specimen, ranging from slight degeneration to full detachment of the labrum (Table 39.2, Fig. 39.5). The control group exhibited one hip joint at 14 weeks of follow-up with malacia of the cartilage and a degenerated labrum. In zone B, neither the operated group, nor the control group showed any signs of cartilage or labral pathology. In zone C, five hip joints from the late follow-up period of 30 to 38 weeks showed malacia in four cases and a full-thickness damage in one case after 38 weeks (Table 39.1). Within the control group there was one case with malacia at the 14-week follow-up period. Regarding labral damage, one case with chondromalacia at 30 weeks of follow-up also showed degeneration of the labrum (Table 39.2), none of the hips in the control group showed labral damage.
Table 39.2 Distribution of Labral Damage Divided by the Acetabular Zonesa | |||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||
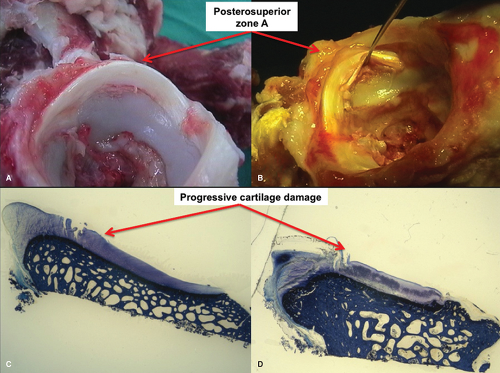 Figure 39.5. The macroscopic specimen of two acetabula obtained after sacrifice are shown in images (A, B)
Get Clinical Tree app for offline access
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|
