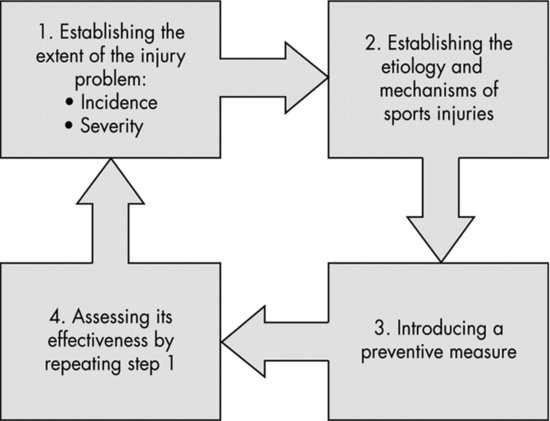
with respect to who is affected by injury, where and when injuries occur, and what is their outcome. The study of the distribution of varying rates of injuries (i.e., who, where, when, what) is referred to as descriptive epidemiology. In the second step, research explores the causes and implications of injury, the why and how of injury. Third, research creates a prevention strategy to reduce the injury burden. In the fourth step, research evaluates the effectiveness of the implemented prevention strategy by reexamining the extent of injury. The study of the determinants of an exhibited distribution of varying rates of injuries (i.e., why and how) and the identification and implementation of preventive strategies is referred to as analytical epidemiology. The focus in this chapter will be on the first two steps of this sequence. A focus on steps three and four will be provided in Chapter 14.
Figure 10.1 Four-step sequence of injury prevention research. (Source: Van Mechelen W., Hlobil H., Kemper J.C.G. (1992) Springer Healthcare © Adis Data Information BV 2012. All rights reserved.)
Descriptive epidemiology
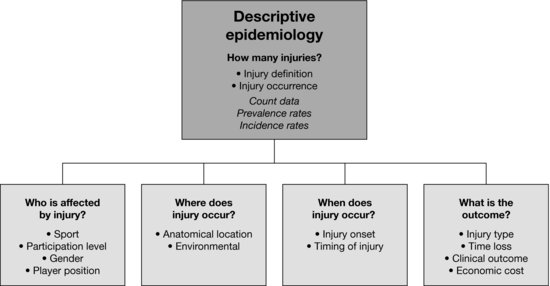
Descriptive epidemiology is by far the most common type of epidemiologic research that has been published in the gymnastics injury literature. A diagram illustrating important aspects of the descriptive epidemiology of sports-related injuries is shown in Figure 10.2 (Caine et al., 2006). These components are discussed below with the purpose of highlighting their various contributions to understanding the incidence and distribution of injury in gymnastics.
How many injuries?
In descriptive epidemiology the researcher attempts to quantify the occurrence of injury. The most basic measure of injury occurrence is a simple count of injured persons. In order to investigate the rate and distribution of injuries it is necessary to know the size of the source population from which the injured individuals were derived, or the population-at-risk. The two most commonly reported rates in the sports injury literature are incidence and prevalence. Prevalence rates pertain to the total number of cases, new or old, that exist in a population at risk at a specific period of time. Prevalence rates published in the gymnastics injury literature typically include rates for specific conditions such as wrist pain and/or radiologic abnormalities of the thoracic-lumbar spine among gymnasts.
The two types of injury incidence most commonly reported in the gymnastics injury literature are clinical incidence and incidence rates. Clinical incidence refers to the number of incident injuries divided by the total number of athletes at risk and usually multiplied by some k value (e.g., 100). In the gymnastics injury literature these rates have most often been presented as injuries per 100 gymnasts. Prior to 1990, clinical incidence was widely reported in the gymnastics injury literature. However, clinical incidence does not account for potential variance in exposure of participants to risk for injury (Knowles et al., 2006). For example, an injured gymnast who is not training in all parts of practice is not at the same risk of sustaining injury as an uninjured gymnast. Incidence rate refers to the number of incident injuries divided by the total time-at-risk and usually multiplied by some k value (e.g., 1000). It is the preferred measure of incidence in research studies because it can accommodate variations in exposure time of individual athletes. Different units of time-at-risk, varying in precision, have been used to calculate incidence rates in the gymnastics literature. These include reporting the number of injuries per k athlete exposures (an athlete exposure or AE is defined as one gymnast participating in one practice or competition in which there is the possibility of sustaining an athletic injury), per k time exposures (one time exposure is typically defined as one gymnast participating in 1 hour of activity in which there is the possibility of sustaining an athletic injury), or per k element exposures (one element exposure is defined as one gymnast participating in one element of activity in which there is the possibility of sustaining a gymnastics injury, e.g., during a vault). Most recent studies on gymnastics injuries report injury rates per k time exposures (e.g., 1000 hours), although there are difficulties associated with this approach, especially with regards to determining time spent competing (O’Kane et al., 2011). Rates expressed per k gymnast exposures have been reported by the National Collegiate Athletic Association injury surveillance system (NCAA ISS) (Marshall et al., 2007). Although attractive in terms of ease of data collection, this approach lacks precision in terms of actual time exposed. A difficulty that may arise in comparing incidence rates from different studies relates to the injury definition employed. A review of the gymnastics injury epidemiology literature reveals that few common operational definitions exist for injury. Definitions include such criteria as presence of a new symptom or complaint, decreased function of a body part or decreased athletic performance, cessation of practice or competition activities, and consultation with medical or training personnel. Defining injury in gymnastics is problematic due to the tendency for gymnasts to train “around” injuries. For example, a gymnast with an ankle injury may continue training on the uneven bars providing she avoids the dismount. Clearly, if injury is defined differently across studies, a meaningful comparison of injury rates is compromised due to different criteria for determining numerator values. Notably, several sports including soccer (football), rugby union, and thoroughbred horse racing have recently published methodological consensus statements that identify definitions and methodology to ensure consistency and comparability of results in studies examining injury in their sports.
Who is injured?
As might be expected, injury rates are most often categorized according to the way in which gymnastics participants are organized for sports (e.g., artistic, rhythmic, or trampoline) or level of sport (e.g., recreational, high school, club college, or international). Given the variance in injury definitions across studies, perhaps the most reliable within- or across-sport comparisons arise from those studies that use a common, exposure-based injury definition and surveillance protocol and where certified athletic trainers or other health professionals record the injury data. Examples include research reports arising from the NCAA ISS and the RIO™ (Reporting Information Online). For example, the NCAA ISS reported a 15-year average of intercollegiate injuries (Hootman et al., 2007). Women’s gymnastics had the second highest rate of competition injuries among women’s intercollegiate sports, preceded by women’s soccer. In practice, women’s gymnastics ranked highest among women’s sports followed by soccer. Unfortunately, there is presently no organized ISS to track and monitor injuries occurring in club gymnastics or at gymnastics schools, which is where most competitive gymnasts train and compete.
Comparison of injury rates across reported studies is difficult given that most authors have not taken into account the exposure to injury risk, but rather reported injury rates per season. Those who did calculate exposure-based overall injury rates reported rates ranging from 0.5 injuries per 1000 hours of participation to 5.3 injuries per 1000 hours of participation for female club gymnasts (Kolt & Caine, 2010; DiFiori & Caine, 2012), which is relatively high and similar to injury rates sustained by girls in sports such as soccer and basketball (Caine et al., 2006). Unfortunately, there are no overall (practice and competition combined) exposure-based injury rates reported for male gymnasts.
There is also a dearth of injury data for participants in Rhythmic and Trampoline Gymnastics. Cupisti et al. (2007) carried out an 8-month prospective study with 70 club-level rhythmic gymnasts aged 13–19 years. They reported 49 significant injuries over the study period, equating to a rate of 1.08 injuries per 1000 hours of training. Whilst Trampoline Gymnastics is a relatively new discipline to the Olympic gymnastics family (since 1998), only one study has reported on the epidemiology of injuries in this sport (Grapton et al., 2012). Based on data gathered by the French Federation of Gymnastics (FFG) over a 5-year period, 226 injuries were incurred in conjunction with trampoline training and competition.
Where does the injury occur?
The “where” of injury distribution involves the anatomical as well as the environmental or situational location (see Figure 10.2). Anatomical locations include body region of injury (e.g., upper extremity) as well as specific body parts (e.g., shoulder or ankle). Identification of commonly injured anatomical locations alerts sports medicine personnel to injury sites in need of special attention during preparticipation musculoskeletal assessment and important “targets” for preventive measures.
Environmental locations provide information on where the injury occurred. Environmental locations reported in the gymnastics injury literature include whether the injury occurred in competition or training; and apparatus used or event, such as balance beam or parallel bars in gymnastics. Information on high-risk injury locations and settings provides important “targets” for further study and preventive measures.
Anatomical location
The lower extremity is the most commonly injured body region for both club-level gymnasts and for high school and college female gymnasts (35.9–70.2% of all injuries) (Kolt & Caine, 2010; O’Kane et al., 2011; DiFiori & Caine, 2012). This finding is not surprising given the repetitive dismounts practiced on the various pieces of gymnastics apparatus. The next most frequently injured region is the upper extremity (7.7–36.0% of all injuries), followed by the trunk and spine (0–43.6% of all injuries), and the head (up to 8.8% of all injuries). A more specific look at these body regions highlights that injuries to the knee are the most common, followed by those to the ankle and the lower back.
The distribution by anatomical location has also been reported in studies of male artistic gymnasts (Kolt & Caine, 2010; DiFiori & Caine, 2012). Similar to that for female gymnasts, the lower extremity was the most injured region (32.8–72.2% of all injuries) in most studies followed by the upper limb (12.5–53.4%) and trunk and spine (7.9–31.3% of all injuries). However, male gymnasts tend to experience a greater proportion of injuries affecting specific upper extremity locations (e.g., shoulder or wrist) than female gymnasts, likely reflecting the skills practiced and apparatus used in men’s gymnastics.
Data on anatomical location of injury is limited for Rhythmic Gymnastics. Cupisti et al. (2004) reported a 10.5% prevalence of low back pain among rhythmic gymnasts compared with 26.0% of matched controls (nongymnasts). In a later study, Cupisti et al. (2007) investigated 70 club-level rhythmic gymnasts over an 8-month period. The most common anatomical sites for injury were the foot (38.3%), knee and lower leg (19.1%), and back (17.0%).
Among competitive trampoline gymnasts the most commonly affected injury sites in one study (Grapton et al., 2012) were the lower limb (49.1%), followed by the spine (32.3%), and upper limb (18.6%). The most frequently injured body parts were knee (19.9%), followed by the lower back (16.8%) and ankle (15.5%).
Environmental location
Not unlike competitive swimming, gymnastics is a sport characterized by long hours of training and repetition and very few hours spent in competition. It is not unusual for some gymnasts, despite training up to 36 hours per week, to participate in only 5–10 competitions per year. It is not unexpected, therefore, that a greater proportion of injuries is associated with training. Several studies of female gymnasts report that 71.0–96.6% of all injuries occur in practice and 3.4–21% in competition (Kolt & Caine, 2010; O’Kane et al., 2011). However, when exposure is accounted for the rate of injury is two to three times greater in competition. For example, collegiate female gymnasts were six times more likely to sustain a knee internal derangement and almost three times more likely to sustain an ankle ligament sprain in competition than in practice (Marshall et al., 2007). Gymnasts are much more likely to participate at a greater intensity in competition than in practice, thus increasing the risk of sustaining an injury. Also, in gymnastics when routines are performed in practice, an effort is made to ensure that the training environment is as safe as possible by performing the routine in smaller pieces, using protective mats and harnesses, and spotting by coaches to a degree not possible in competition (O’Kane et al., 2011). Other factors possibly contributing to higher competition injury rates include higher pressure to perform, travel, and the different equipment and environment inherent in traveling to a competition (O’Kane et al., 2011). Given the higher rate of injury during competition, an increased focus and analysis of risk factors and preventive measures associated with competition injuries is required.
No studies of injury in Rhythmic or Trampoline Gymnastics have examined injury data in relation to whether injury occurred during training or competition.
With gymnasts participating in a wide variety of events or apparatus (six for men, four for women, and many other nonapparatus training drills), it is important to understand where the greatest risk of injury lies. However, it is difficult to fully understand the relationship between gymnastic event and injury because most research reports a percentage distribution of injury by event, and therefore does not account for time exposed. It is likely that the incidence rate of injury would be greatest during floor routines in Artistic Gymnastics due to the high frequency of dismounts and landings. However, this hypothesis awaits confirmation from exposure-based research.
In Men’s Artistic Gymnastics and Rhythmic and Trampoline Gymnastics, exposure-based data in relation to event are not available in the published literature.
When does injury occur?
As Figure 10.2 indicates, the next characteristic of injury distribution is the when of injury occurrence. Time factors are typically expressed in terms of injury onset and timing of injury.
Injury onset
There are two broad categories of injury onset that differ markedly in etiology. Overuse injuries are more subtle and develop gradually over time. They are the result of repetitive microtrauma to the tendons, bones, and joints. Common examples include growth plate injuries, patellar tendinosis, and medial tibial stress syndrome. Injuries that occur suddenly are often termed acute or sudden impact injuries and are usually the result of a single, traumatic event. Common examples include wrist fractures, ankle sprains, and shoulder dislocations. An injury history may actually involve both categories of injury onset, such as when an acute injury is superimposed on a chronic mechanism. However, this third injury category is not often distinguished in the epidemiologic literature on gymnastics injuries. Most studies in the gymnastics injury literature do not distinguish between acute and overuse injuries. However, this is an important oversight since risk factors for overuse and acute injuries may differ. Determination of activity or apparatus at the time of injury should be limited to acute injuries (O’Kane et al., 2011). The importance of identifying injury onset is also important given the growing evidence of overuse problems in gymnastics, particularly among child and adolescent gymnasts.
In gymnastics, where a high number of training hours are required for high-level performance, and where a number of high-risk skills are performed, it is expected that both overuse and acute injuries will occur. Studies reporting injury onset for female gymnasts indicate a range of 21.9–55.8% for overuse and 44.2–82.3% for acute injuries (Kolt & Caine, 2010; O’Kane et al., 2011). O’Kane et al. (2011) reported incidence rates of 1.8 and 1.3 injuries per 1000 hours for overuse and acute injuries, respectively.
Studies of male gymnasts also show a greater proportion of sudden versus gradual onset injuries (Kolt & Caine, 2010). The proportion of overuse versus acute injuries may vary according to anatomical location and competitive level with advanced-level gymnasts showing a higher proportion of overuse injuries in some studies.
The main injury study in Rhythmic Gymnastics to date (Cupisti et al., 2007) did not report the onset of injury as overuse or acute.
Timing of injury
Examples of timing of injury include time into practice, time of day, and time of season when injury occurs. It stands to reason that if rates are higher during a particular time, then efforts to better understand the risk factors for increased incidence are in order. For example, if the proportion or incidence rate of injuries is shown to be greater during the latter part of a training session or competition, or when the gymnast has been on an apparatus for an extended period of time, then fatigue and possible loss of concentration could be considered as possible contributing factors.
When examining timing of injury, both timing within a practice session and timing during a year-long season are important. Several studies have reported that the early part of a training session or competition is a period where a relatively high frequency of injury occurred (Kolt & Caine, 2010) suggesting insufficient warm-up.
Several studies have also followed the time into the season for injury occurrence in women’s gymnastics. These findings indicate that injury rates can increase following periods of decreased training, during periods of practice of competitive routines, during weeks just prior to and during competition, and during competitive seasons (Kolt & Caine, 2010).
What is the outcome of injury?
As Figure 10.2 indicates, the next characteristic of injury distribution is injury outcome related to severity, or the “what” of injury occurrence. Injury severity can span a broad spectrum from abrasions to fractures, to those injuries that result in severe permanent functional disability (i.e., direct catastrophic injury). In the epidemiologic literature on sports injuries, injury severity is typically indicated by one or more of the following: injury type, time loss, need for medical treatment, and residual symptoms. Assessment in each of these areas is important to describe the extent of the injury problem. It may be, for example, that injury incidence is similar in two sports; however, the severity of injury may vary considerably between these sports.
Injury type
Identification of common injury types is important because it alerts sports medicine personnel to injury types in need of special attention and it directs researchers in identifying and testing related risk factors and preventive measures. Most gymnastics injury studies report injury types in general terms such as contusion or fracture, with few specifics on type of fracture, grade of injury, and so forth. Injury types are generally reported as percentage values. However, it would be preferable to report incidence rates for specific injury types, for example, anterior cruciate ligament (ACL) injuries, to better facilitate the analysis of risk factors and preventive measures.
Injury types in gymnastics have been categorized differently across studies, making comparison difficult. For example, some studies combine lower leg and ankle injuries, while others separate these injury types. A recent review of injury types in gymnastics (Kolt & Caine, 2010) indicates that sprains (15.9–43.6%) are the most common type of injury followed by strains (6.4–31.8%). Typically caused by inversion ankle injuries, ankle ligament sprains are the most common acute injuries in gymnastics (DiFiori & Caine, 2012). Other types of injuries that are common include contusions, fractures, and inflammatory conditions.
Although pain may not necessarily result in time loss and/or injury, pain among gymnasts is problematic and may affect performance. Many gymnasts continue training and competing with pain. For example, Caine and Nassar (2005) reported that injuries or conditions treated at the 2002–2004 USA Gymnastics National Women’s Artistic Championships ranged from 27.6 to 80% of the junior and from 62.5 to 70% of senior gymnasts. Next to sprains (27.4%), the most common treatments were for overuse conditions (17.8%) and nonspecific pain (14.4%). Similarly, Harringe et al. (2004) noted that half of the team gymnasts (58%) in their study competed despite having symptoms from an injury on the day of competition.
Wrist pain is common among gymnasts of both sexes who train and compete at advanced skill levels. Prevalence estimates of wrist pain among these participants range from 46 to 79% (DiFiori & Caine, 2012). Chronic wrist pain in young gymnasts does not appear to be a transient phenomenon and may result in stress-related injury (e.g., stress changes to the distal radial physis). Prevalence studies also indicate that low back pain may be common among artistic gymnasts; however, these data arise from cross-sectional studies published more than 20 years ago (Caine et al., 1996). Radiological findings indicate the potential damaging effects of excessive mechanical loading on the immature spine of gymnasts including damage to the pars interarticularis resulting in spondylolyis or spondylolisthesis, discogenic pathology, and vertebral endplate abnormalities (Caine et al., 1996). However, several researchers have suggested that anterior column spine problems, such as anterior vertebral endplate fractures, are becoming more common than posterior column spine problems (Caine & Nassar, 2005; Marshall et al., 2007).
In prior literature, the frequency of head injuries and concussion is quite low, ranging from 0 to 0.7% among female artistic gymnasts (Caine & Nassar, 2005), and 2.3% of practice injuries and 2.6% of competition injuries among collegiate female gymnasts (Marshall et al., 2007). However, in the most recent study published on Women’s Artistic Gymnastics injuries (O’Kane et al., 2011), the percentage of gymnasts reporting head injury was 8.8%, and a history of concussion ranged from 15.6 to 30.2% depending on the definition of concussion.
The data on injury types for male gymnasts are scanty, but indicate a similar distribution to that experienced by female artistic gymnasts.
For Rhythmic Gymnastics, only one study has reported injury type (Cupisti et al., 2007). They found that, of the 46 injuries recorded, 26.1% were strains, 15.2% sprains, 17.4% contusions, 6.5% fractures, 2.2% dislocations, and 32.6% were classified as other. Injury types among competitive Trampoline Gymnastics (Grapton et al., 2012) are mainly ligament sprains (44.2%) affecting the lower limb, followed by bone (31.9%) and muscular injuries (18.6%). The most frequently injured body parts were knee (19.9%), followed by the lower back (16.8%) and ankle (15.5%).
Time loss
A useful measure of injury severity used in the literature on gymnastics injuries is the duration of restriction from athletic performance subsequent to injury. Understanding the time lost to training or competition as a result of injury is important for coaches, sports medicine personnel, and participants. Not only does it provide an indication of the severity of injury, but also the impact that the injury has on overall training and competition programs. Most studies reporting time loss use days lost from practice or competition as a measure of injury severity. These time loss data are often categorized by time periods (e.g., 7 or less days) indicating degree of severity. Although the use of days lost from participation may be among the more precise representations of injury severity in the literature, this approach is not without problems. For example, subjective factors, such as personal motivation, peer influence, or coaching staff reluctance/encouragement, may determine if and when gymnasts return to practice or competition. Accessibility to a health care professional and location of injury may also impact decision of when to return to gymnastics. As noted previously, it is not uncommon for gymnasts to participate at competitions with chronic injury problems (Harringe et al., 2004; Caine & Nassar, 2005).
Gymnastics is a sport characterized by very little total time loss from full participation. That is, in the presence of most injuries, participants can continue to train in a modified manner or on apparatus or skills that do not impact on the injured body part. In many cases this is important as a method to maintain skill and fitness levels. Although most gymnastics injuries are relatively minor in terms of time loss, there is some research that indicates that particularly advanced level gymnasts may spend a substantial portion of their training at less that full practice (Kolt & Caine, 2010). For example, over 16 years, 39% of all women’s intercollegiate competition injuries and 32% of all training injuries resulted in a time loss of 10 or more days (Marshall et al., 2007).
For competitive rhythmic gymnasts, Cupisti et al. (2007) found that for each injury sustained, 4.1 training sessions were missed and 32 were modified.
Need for medical treatment
There are few data published that provide an insight into the number of gymnasts who seek medical attention for injury and the cost of this treatment. As mentioned above, 27.6–80% of the junior and from 62.5 to 70% of senior gymnasts, respectively, were treated for pain or injury at the USA National Women’s Artistic Championships between 2002 and 2004 (Caine & Nassar, 2005). During a 1-year injury surveillance of advanced club-level female gymnasts, 36 of 50 gymnasts consulted with a physician for 59 injuries (Caine et al., 1989).
Clinical outcome
Clinical outcome of injury includes such factors as recurrent injury, nonparticipation, and residual effects. An unfortunate outcome of many injuries, at all levels of sport, is recurrent injury. Gymnastics is a sport where participants experience recurrent injuries for several reasons including premature return to activity, inadequate rehabilitation, and underestimation of the severity of the primary injury. A gymnast with previous injury who returns to participation may be characterized by a changed injury risk profile, particularly if the original injury has not been properly rehabilitated. In studies of competitive female artistic gymnasts between 24.5 and 32.3% of all injuries were reinjuries (Kolt & Caine, 2010). No recent published data are available on rates of recurrent injury, nor are there any data available for male artistic gymnasts.
Another important but infrequently researched aspect of injury outcome relates to the frequency of season- or career-ending injuries (i.e., nonparticipation). An important question to address is how many gymnasts drop out of their sport, either temporarily or permanently due to injury. Data on season-ending injuries have been provided in only a few studies of young gymnasts. The types of injuries that were involved in decisions to drop out included ACL rupture, osteochondritis dissecans of the elbow, knee meniscus lesions (although these are now more easily managed with arthroscopic treatment), navicular stress fracture, chronic rotator cuff conditions, and injuries to the low back. Other studies that have examined the relationship between injury and dropping out of sport found that between 16.3 and 52.4% of those who dropped out of club-level gymnastics had an injury at the time of withdrawing from the sport (Kolt & Caine, 2010). Although this may suggest that injury played a role in the withdrawal, there are several other factors (e.g., age, transition to other sports, or loss of motivation or interest) that could have influenced this decision. Notably, O’Kane et al. (2011) reported that a little more than half of the gymnasts in their study played other sports.
Perhaps the most important question one can ask related to injury severity concerns residual or long-term effects of injury. Although engaging in physical activity has many health benefits, there is also risk of injury that may have long-term consequences on the musculoskeletal system resulting in reduced levels of physical activity or medical treatment. If residual symptoms are slight, they may cause the gymnast to modify his or her level of training. In some cases, however, functional limitations resulting from injury may preclude further participation in gymnastics or, following participation, result in reduced levels of activity secondary to residue from injury. For example, a link between acute knee or ankle injury and osteoarthritis is likely. Several studies found no differences between former gymnasts and control groups (nongymnasts) in back pain, but reported a higher prevalence in radiological changes (e.g., degenerative changes) in the gymnastic groups (Kolt & Caine, 2010).
In extreme cases, such as catastrophic injury, serious physical damage may result in permanent, severe functional disability such as quadriplegia. There is concern in gymnastics regarding catastrophic injury given the “high-risk” skills being trained and competed. The limited data on catastrophic injuries in gymnastics arise from case reports and series from the United Kingdom, China, the United States, Japan, and Germany (Kolt & Caine, 2010) and include those injuries suffered in Trampoline Gymnastics. Data arising from the National Center for Catastrophic Sports Injury Research (http://www.unc.edu/depts/nccsi/; accessed on February 22, 2013), which has tracked catastrophic injuries in high school and college settings since 1982, indicate a total of 20 direct catastrophic injuries that occurred among high school (n = 13) and college (n = 7) gymnasts during 1982–2011. Catastrophic injury rates (per 100,000 participants) were relatively high in gymnastics compared to other sports. In contrast, data arising from multiple cohort studies of club-level and recreational gymnasts indicate no catastrophic injuries (Kolt & Caine, 2010).
The Cupisti et al. (2007) study of Rhythmic Gymnastics did not identify any catastrophic injuries.
Analytical epidemiology
Analysis of gymnastics injury risk factors has produced a number of significant injury predictors—including such factors as age, competition, periods of rapid growth, previous injury, and stressful life events—which have shown consistent results across multiple studies. However, much of the analytical literature suffers from one or more of the following limitations: injury definitions and methods of injury data collection that are extremely variable, incidence rates based on clinical incidence rather than incidence rates (i.e., rates based on hours or sessions of exposure) are often used to distinguish high-risk athletes, failure to account for the different categories of injury onset, and inappropriate analyses for detecting multifactorial risks. As a result, much of the risk factor research should be viewed as initial work in the important search for injury predictors and that may provide interesting variables for manipulation in other study designs.
Injury risk factors
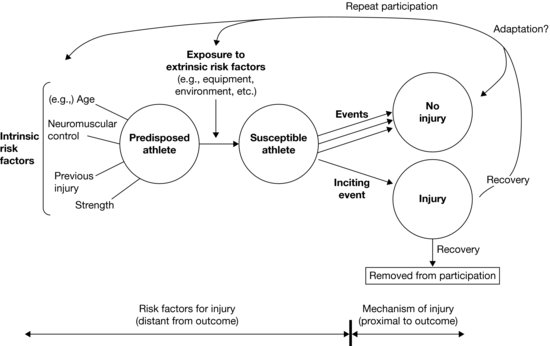
For injury intervention and rehabilitation programs to be effective, an in-depth knowledge of injury risk factors is paramount. This is particularly so given that gymnastics is a sport with relatively high injury rates. Risk factors may be classified as intrinsic or extrinsic. Intrinsic factors are individual biological and psychosocial characteristics predisposing a person to the outcome of injury such as previous injury, strength, or life stress. Extrinsic (or enabling) risk factors are factors that have an impact on the gymnast “from without” and include such factors as coach’s qualifications, training time, and level of competition. Intrinsic and extrinsic risk factors may interact to increase the risk of injury.
Risk factors can also be divided into modifiable and nonmodifiable factors. Modifiable risk factors refer to those that can be altered by injury prevention strategies to reduce injury rates. Although nonmodifiable risk factors such as gender or age may be important considerations in many studies of injury prediction and should be accounted for in statistical analyses, it is above all important to study factors that are potentially modifiable. What complicates the identification and quantification of risks is that causality associated with injury is both extremely complex and dynamic in nature. Willem Meeuwisse et al. (2007) proposed a dynamic recursive model that accommodates a multifactorial assessment of causation in athletic injuries and emphasizes the fact that adaptations occur within the context of repeated participation in sport (both in the presence and absence of injury) that alter risk and affect etiology in a dynamic, recursive fashion (see Figure 10.3). In this model, intrinsic factors are viewed as factors that predispose the athlete to react in a specific manner to an injury situation. However, what is important to understand is that intrinsic factors are not constant and may change in response to injury or to absence of injury (i.e., adaptive changes such as increased intrinsic strength).
< div class='tao-gold-member'>