Fig. 32.1
A simple articular fracture of the radial and ulnar styloid, fixation with percutaneous Kirschner wires
Percutaneous pins alone cannot provide sufficient stability to prevent recurrent dislocations. Their use is always associated with the application of a splint or an external fixator, in the so-called augmented external fixation described later.
Pin fixation is also the preferred surgical method for the treatment of fractures in children [28, 29] in cases where conservative treatment is unsuccessful.
32.6.4 The Role of External Fixation
External fixation has been considered an important means of treatment in the past years, as internal fixation devices were not as stable and versatile as they are today [30].
More recently, external fixation has retained a role in selected situations where extreme comminution, massive damage or loss of skin and soft tissue, critical survival conditions in trauma, and contamination of exposed bone discourage the use of internal fixation implants.
In many cases, external fixation is performed as a temporary stabilizer, and the treatment shifts to ORIF as adverse conditions are resolved.
In very comminuted fractures, where stability of internal fixation devices is not granted, external fixation may be associated in order to enhance stability in the early phases of bone healing [31].
The maintenance of reduction with external fixators is often based on distraction that may lead to adverse conditions such as ligament lesions, CRPS, and secondary hypercorrection [32].
The combination of external fixation devices with K-wires (augmented external fixation) enhances stability, prevents secondary displacement, and reduces the need for distraction and related complications [33] (Fig. 32.2).
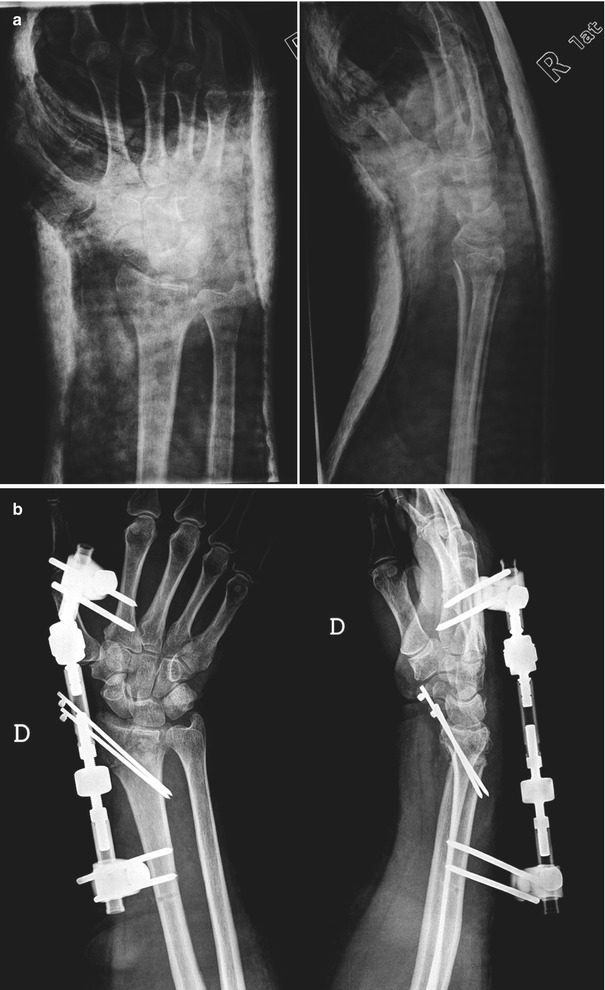
Fig. 32.2
Extra-articular fracture with radial translation of the distal epiphysis. (a) Cast immobilization fails in controlling the translation. (b) Reduction and stabilization with augmented external fixation
32.6.5 The Role of Arthroscopy
Arthroscopy is considered an important means in the treatment of articular comminuted fractures of the wrist [34].
Arthroscopic assistance allows direct visualization of the ongoing reduction of articular fragments and a more accurate reconstruction of the joint surface, which greatly affect the outcome of medium- and long-term results.
Arthroscopy is also useful in the early evaluation and treatment of associated ligament lesions such as scapholunate or lunotriquetral ligaments or TFC [20]. These lesions may be underestimated during the assessment of the injury, as pain and deformity does not allow to adequately examine these articular structures, and stable or incomplete ligament tears often go undetected by standard x-rays and CT scan. Once detected, ligament tears associated to the fractures can be immediately repaired arthroscopically or by an open approach.
Wolfe [22] recommends postponing arthroscopic reduction for 3–7 days to avoid excessive bleeding, which may limit visibility, and risk development of a compartment syndrome due to extravasation of fluids into the soft tissues.
Arthroscopic reduction is followed by stabilization of the fracture by percutaneous pins or internal plate fixation.
32.6.6 The Role of Internal Fixation
For many years, internal fixation of distal radius fractures was affected by a high rate of complications due to the interference of implants with contiguous structures, in particular the extensor tendons, and to the rather poor stability of traditional fixation systems applied to osteoporotic or fragmented metaphyseal bone.
For these reasons, internal fixation used to be limited to those fractures considered untreatable by other means.
The development of a safe volar approach to the distal radial epiphysis [35] and the availability of fixed angle plates have dramatically changed surgical treatment of distal radius fractures. Metaphyseal comminution is a significant cause of instability. A great variety of devices has been developed for the treatment of distal radius fractures. Screws secured to the plate buttress the subchondral bone and prevent secondary displacement of the joint surface [36, 37]. The possibility to fix the screws to the plate at variable angles of last generation fixation devices has permitted a more reliable control of bone fragments in complex fractures and a better restoration of anatomy.
Low-profile and less invasive dorsal plates, designed for specific bone fragments, are used alone or in combination with volar plates when they are unable to maintain the obtained reduction of dorsal fragments alone [10].
32.6.6.1 Dorsal Approach
The dorsal epiphysis of the radius is approached by opening the third retinacular canal and elevating the retinaculum on both sides without exposing the extensors. Care must be taken in extensive comminution to preserve small bone fragments that tend to follow the elevated soft tissues.
Dorsal fixation of distal radius fractures has evolved during the last decades from plates applied to the whole dorsal surface of the distal epiphysis, to smaller low-profile plates designed for specific column fractures [10] (Fig. 32.3). Despite this evolution, interference with extensor tendons may still occur, and dorsal fixation is indicated only in those cases where a volar approach alone fails to restore anatomical conditions.

Fig. 32.3
Radial column fracture fixation with a dorsal specific fragment plate and screws
A dorsal approach can also be exploited to control “difficult” dorsal fragments that can be then fixed with a volar plate alone or in combination with dorsal screws or plates once reduced [38].
32.6.6.2 Volar Approach
The volar aspect of the distal radius is easily exposed with different approaches [35]. The pronator quadratus muscle is gently detached and elevated from the radial metaphysis. The brachioradialis can be separated to facilitate the reduction of fractures involving the radial styloid. Articular fragments must be repositioned under direct view, arthroscopic, or fluoroscopic control. In cases with extensive metaphyseal comminution, bone grafts or bone substitutes can contribute to restore bone continuity and support subchondral bone and articular fragments. Once the fracture is reduced, a temporary stabilization with Kirschner wires can facilitate the positioning of a volar plate.
Most last generation plates have been designed to be placed proximally to the watershed line to prevent interference with flexor tendons. Locking and traditional screws can be chosen to achieve a better stabilization of every fracture, buttress subchondral bone, and pull dorsal fragments (Fig. 32.4). The repositioned pronator quadratus muscle covers the plate and protects the flexor tendons.
Fig. 32.4




Articular fracture of the distal radius. (a) Standard x-rays. (b) CT adds important information about the number and pattern of fragments. (c) Fixation by means of a volar locking plate positioned proximal to the watershed line
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
