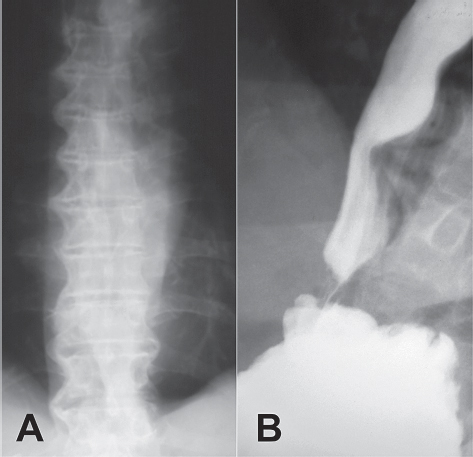
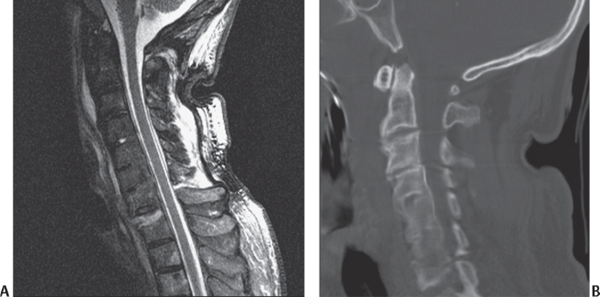
26 Diffuse idiopathic skeletal hyperostosis (DISH), or Forestier disease, is a fairly common (up to 28% of elderly patients) degenerative disorder of unknown etiology, affecting mostly older patients (45 to 85 years old) and men (65%) more than women. It was first described in 1950 as a disorder characterized by spinal stiffness, osteophytosis, and “flowing” new bone formation along the margins of the thoracic spine (Fig. 26.1A). The anterior longitudinal ligament (ALL) is usually most involved. Although the disease is more prevalent in certain families, no clear genetic association with the human leukocyte antigen (HLA) system has been identified, and no relationships have been found with either rheumatoid arthritis or ankylosing spondylitis (AS), with which it is often confused. DISH can be associated with type II diabetes, obesity, biliary stones, atheromatous vascular disorders, hypertension, and lipid and purine metabolism disorders. DISH is characterized by ossification of the ligamentous insertions (fibro-osteosis) and ossification/calcification of tendons, ligaments, and fascia in both the axial and the appendicular skeleton. This is caused by invasion of blood vessels into cartilage and differentiation of pluripotent cells into osteoblasts. The most common symptoms of DISH are spinal rigidity and decreased joint mobility with occasional dysphagia from esophagus compression (Fig. 26.1B). Pain and nerve root irritation due to narrowing of the vertebral foramina rarely occur, but spinal cord compression secondary to ossification of the posterior longitudinal ligament (OPLL; see Chapter 22) can cause myelopathy. The diagnostic criteria for DISH include (1) flowing ossifications along the anterolateral aspect of at least four thoracic vertebrae, (2) absence of (Fig. 26.1A) facet-joint ankylosis or sacroiliac sclerosis (these criteria belong to AS; see Chapter 25), and (3) conservation of intervertebral disk height between involved segments. Fig. 26.1 (A) Characteristic chest X-ray finding of “flowing” bone on the right side of the thoracic spinal column. (B) Dysphagia due to a large diffuse idiopathic skeletal hyperostosis–anterior osteophyte compressing the esophagus. Most patients are asymptomatic or have short episodes of “periarthritis” due to activation of the enthesopathy process. For the spine, patients usually have a history of stiffness upon forward bending and mild to moderate pain in the mid-back region. Complaints are fairly nonspecific, but radiographic findings may be dramatic. DISH is often discovered incidentally and is predominantly a radiographic diagnosis. The T7 to T11 levels are most frequently involved, and the changes are often visible even on a chest radiograph. Extraarticular ankyloses take the form of flowing candle wax in DISH, as opposed to the vertically oriented osteophytes in the “bamboo spine” that form intraarticular ankyloses in AS (see Chapter 25). Disk space narrowing is minimal, and the facet joints are usually preserved. A bone scan generally shows increased uptake and can raise the suspicion of a malignancy. Axial computed tomography (CT) cuts show a thin radiotransparent band between the calcified ALL and the vertebral body wall on the right side of the anterior spine. Because no specific drug therapy has been discovered, simple analgesics or nonsteroidal anti-inflammatory drugs (NSAIDs) are usually prescribed. Improved flexibility and activities of daily living were successfully maintained for up to 2 years after the end of an active rehabilitation program. Cases associated with symptomatic stenosis may require surgical decompression. Patients suffering from DISH are at high risk for spinal fractures. Delayed diagnosis is frequent because the trauma is often trivial. Hyperextension injuries occur most frequently through an entire vertebral body or through a disk space in between the ankylosed segments; the incidence of neurologic compromise is relatively high. The long lever arm that develops as a consequence of the ankylosis of multiple vertebral elements causes fractures to displace easily. Back and neck pain after minor trauma in a patient with DISH need to be worked up with a high index of suspicion for fracture. Involved areas need to be imaged (Fig. 26.2A,B) with either CT or magnetic resonance imaging (MRI) to rule out global spinal instability, because this is usually underrepresented on plain radiographs. Fig. 26.2 Sagittal (A) MRI and (B) CT reconstruction in DISH patient after motorcycle accident showing three-column bone injury at the cervico-thoracic junction with minimal soft-tissue damage. These patients are at extreme risk of becoming paralyzed if the diagnosis is missed. Halo immobilization is strongly recommended pending surgical stabilization.
Diffuse Idiopathic Skeletal Hyperostosis
![]() Classification
Classification
![]() Workup
Workup
History
Spinal Imaging
![]() Treatment
Treatment
![]() Outcome
Outcome
![]() Complications
Complications
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


