Chapter
8
Deformity Correction: Foot and Ankle
Planning, persistence and passion are three pillars of foot and ankle deformity correction!
This chapter describes the following commonly seen foot and ankle deformities in adult population.
♦ Sagittal plane deformities
• Equinus
• Dorsiflexion contracture
♦ Coronal plane deformities
• Ankle varus
• Ankle valgus
♦ Cavus
Evaluation of Foot and Ankle Deformity
The criteria for evaluation of foot and ankle deformities are listed below.
♦ Age and occupation
♦ Activity level
♦ Duration
♦ Causes: Posttraumatic, congenital, acquired and degenerative
♦ Comorbid conditions
♦ Joints above: Knee, hip, and spine
♦ Joints proximal
♦ Joints distal
♦ Neurological status of the limb
♦ Vascular status of the limb
♦ Pressure points
♦ Skin and scars
♦ Presence of implants
♦ Presence of infection
♦ Soft tissue contractures: Tendo Achilles contracture is the most common
♦ Bone quality
Principles of Deformity Correction
♦ The aim is to achieve a plantigrade foot
♦ Correction proceeds from proximal to distal
♦ Soft tissue releases must precede bony correction
♦ Bony corrective procedures must precede tendon transfer
♦ Removal of bone for deformity correction must precede removal of articular cartilage at corrective arthrodesis
♦ In all indicated cases, supportive braces and orthotics must be planned and explained to a patient well in advance
Equinus Deformity
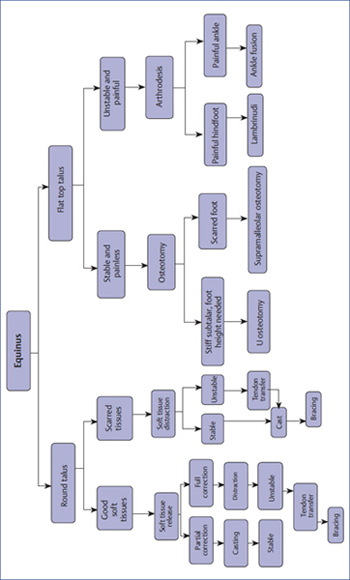
Management of equinus varies as regards the shape of talus, which is illustrated in Flowchart 8.1.
Tips and Tricks
The following points are needed to be considered for managing the equinus deformity:
♦ By flexing the knee, if the equinus is correctible either completely or partially, it signifies that the gastro-soleus is tight as it relaxes on knee flexion. If the deformity corrects completely on knee flexion, it is possible that a percutaneous tendo Achilles release may completely correct the deformity.
♦ White slide technique for percutaneous tendo Achilles release: Distal medial, middle lateral, and proximal medial incisions at the interval of few inches between them are made. The distal-most incision is taken a few inches above the tendo Achilles insertion. This is followed by forced ankle stretching in dorsiflexion and casting is put for 3 to 6 weeks.
♦ Take care not to damage the saphenous vein and sural nerve during this procedure.
♦ The incisions need to be modified as per the association of heel varus or valgus together with equinus, where, respectively, two medial, and one lateral incisions for heel varus and two lateral and one medial incisions for heel valgus are used.
♦ First choice is always to release posterior soft tissues.
♦ On lateral X-ray, presence of a round dome talus suggests that correction of equinus deformity is possible within ankle alone.
♦ If upon knee flexion the deformity is partially correctible, it may mean that not only is the tendo Achilles contracted, but also are some of the posterior soft tissues around the ankle. This needs posterolateral soft tissue release.
♦ Important structures that need release are on the posterolateral aspect rather than on the posteromedial aspect.
Posterolateral Release
A small curvilinear incision is made starting proximally and medially, crossing over the tendo Achilles, which ends with a gentle curve posterolaterally below the lateral malleolus. The paratenon of the tendo Achilles is neatly and carefully incised to prevent damage. A vertical split is made in the substance of the tendo Achilles. At its distal end the medial edge is cut, and at its proximal end the lateral edge is cut. Dorsiflexing the ankle will give some correction. Now the retractors are placed on the inner edges of the cut tendo Achilles and the edges are separated to gain deeper entry. The deep fascia is cut and the fat juts out. The flexor hallucis longus (FHL) tendon and muscle belly are retracted from the lateral side by the scalpel handle and retracted medially. The tendon of the FHL is key to saving the neurovascular structures at the posterior end of the ankle. It is visualized and retracted medially, taking the artery and nerve along with it.
This gives access to the entire posterior aspect of the ankle. The ankle capsule is released with a knife. In large deformities, the subtalar capsule may also be released. The lateral malleolus is palpated, and the knife is slid gently from distal to proximal in a gently curving arc to release the posterior syndesmotic ligament. As the anterior aspect of the talus is broader than the posterior one, sliding into the ankle mortise would not be possible unless the syndesmotic ligament is released, allowing the fibula to spring apart and allow the broader anterior part to extend into the tibio-talar joint.
The knife is now kept adjacent to the calcaneus and slid down laterally, releasing the calcaneofibular ligament. This ligament tethers the calcaneal tuberosity proximally and does not allow it to migrate distally unless released. This completes the soft tissue release and full correction may be achieved.
If correction is not fully achieved, it may indicate that tendons of the tibialis posterior and flexor digitorum longus are tight. After retracting the neurovascular bundle laterally, they are visible under the deep fascia through the proximal part of the wound. Z lengthening is performed of both the tendons and they are sutured. We preserve its paratenon by not going either medial or lateral to the tendo Achilles and ensure that there is no skin necrosis and wound dehiscence.
Soft Tissue Distraction
With a rounded talus but posterior soft tissues that may not be healthy or pliable, we can achieve correction with soft tissue distraction.
♦ The Ilizarov fixator is an ideal tool and has comprehensive capabilities under all clinical circumstances to achieve full correction
♦ A limited soft tissue release should be performed posterolaterally to achieve some correction before applying Ilizarov apparatus
♦ The Ilizarov fixator is mounted with two rings on the tibia, with two half pins and wires
♦ Configuration for the foot fixation depends on whether the equinus deformity is accompanied by cavus or varus or valgus or presence of deformity between the hindfoot and forefoot
Ilizarov Fixator Application
If there is no deformity within the foot, a horseshoe-shaped ring is used for foot fixation. A half pin is inserted in the calcaneum from the tuberosity from posterior to the anterior. One or two olive wires are inserted in the calcaneum from the posteromedial aspect from behind the neurovascular structures to exit laterally and distally. This may be sufficient fixation for the hindfoot. In more rigid deformities, additional wire is inserted from the anteromedial direction to engage in the sustentaculum, just underneath the tendons but dorsal to the neurovascular structures to exit posterolaterally. These two wires subtend a right angle to each other and hence offer very strong fixation.
At least two more wires are inserted in the mid- and forefoot. An olive wire from lateral aspect is inserted through the cuneiforms to exit medially. Just proximal to the MTP joints, an olive wire is inserted from medial side into the first metatarsal, passing underneath the second and the third and exiting laterally through the substance of the fourth and fifth metatarsals.
A wire is also inserted in the head–neck junction of the talus and an olive wire is inserted from the lateral side. This offers control over the talus. After tensioning, the foot frame becomes rigid.
Soft Tissue Distraction
Soft tissue distraction at the ankle may be performed using two principles:
1) Constrained correction
2) Unconstrained correction
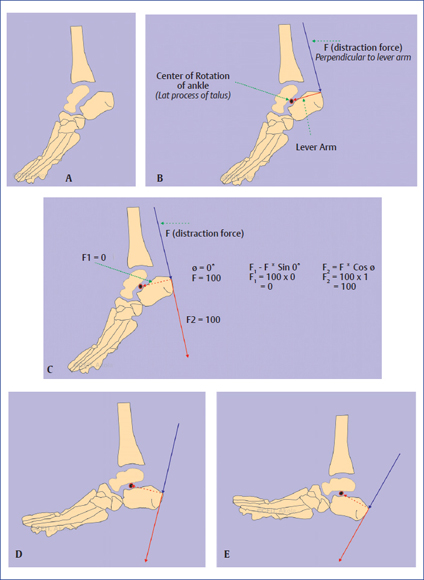
Principle of correction of equinus by distraction is shown in Fig. 8.1A to E.
Constrained Correction
We may constrain the correction to occur around hinges placed in the apparatus. The center of rotation of the ankle is located around the lateral process of the talus. If we can locate the medial and lateral hinges to overlap accurately at this level, we can place the posterior distraction motor rods posteriorly anywhere conveniently. The rate of distraction is calculated depending on the distance between the posterior rods and hinge locations. The anterior rods do not perform compression. They are kept in “passive” mode; however, they are loosened just prior to posterior distraction and then locked in any new (slightly changed) position.
The distraction process is monitored with anteroposterior (AP) and lateral (LAT) X-rays to ensure that the tibio-talar joint remains congruent, that it is not overdistracted, and that cartilage is not crushed at the joint level.
Once correction is achieved, we aim to achieve overcorrection by a few degrees into dorsiflexion. The apparatus is maintained for a few more weeks in this mode. Extensions are made to the apparatus to enable the patient to walk with almost full weight bearing. After the apparatus is removed, a walking cast is applied for a few weeks and a brace is made to be worn at night to ensure there is no recurrence of deformity.
Equinus deformity in a patient who is treated with constrained correction is serially depicted in Fig. 8.2A to G.

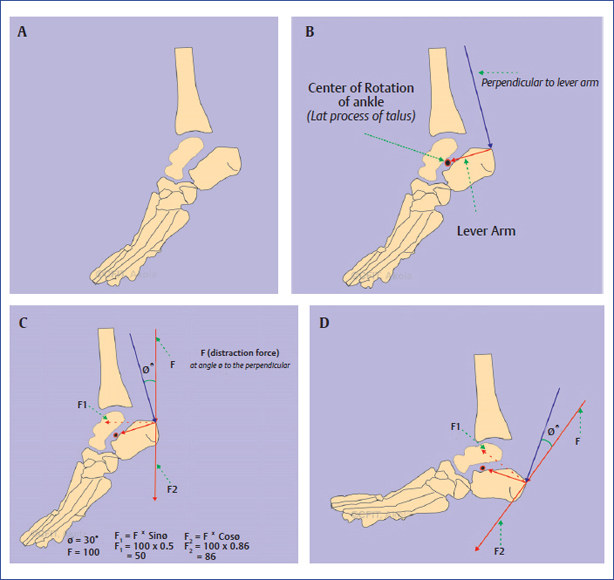
Principles of correction of equinus by subluxation are shown in Fig. 8.3A to D.
Equinus deformity in a patient who is treated with equinocavus distraction is serially depicted in Fig. 8.4A to K.


Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


