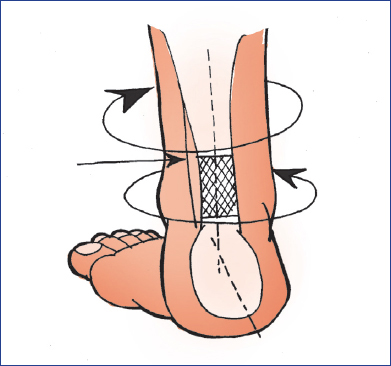
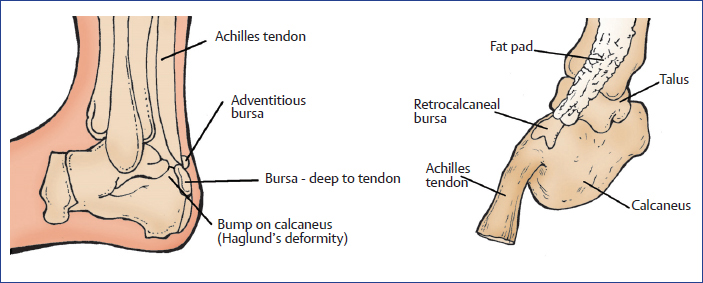
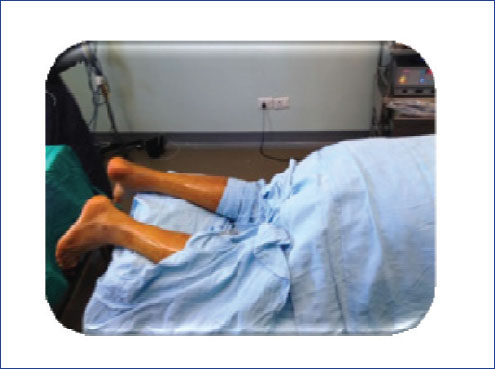
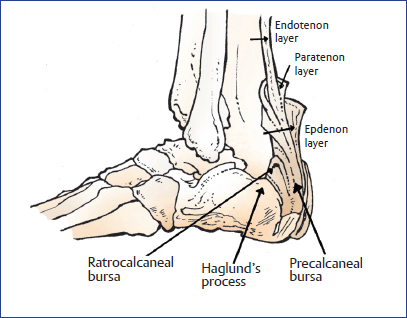
Chapter Tendo Achilles is the strongest tendon of body contributing significantly in gait cycle! The following are the common disorders of tendo Achilles tendon: ♦ Acute rupture ♦ Chronic (neglected) rupture ♦ Noninsertional tendo Achilles tendinopathy ♦ Insertional tendo Achilles tendinopathy: Tendon problems, bursal problems, bony spurs, and ruptures Typical anatomical considerations for disorders of tendo Achilles tendon include the following: ♦ Tendon twists 90 degrees onto itself at insertion so gastrocnemius inserts posterolaterally and soleus inserts posteromedially (Fig. 15.1). ♦ Tensioning in twisted fibers causes “wringing effect,” compromising blood flow, promoting ischemic degeneration. ♦ Tendon has a very thin paratenon (Fig. 15.2). Fig. 15.2 Tendon has a thin paratenon with wringing effect. ♦ Tendon inserts slightly medially on heel inverting it on its action. ♦ Insertion of Achilles: Half way between the dorsal and plantar aspects of the posterior tuberosity. ♦ Tendon has two bursas at insertion: Retrocalcaneal bursa in front and Achilles tendon bursa behind (Fig. 15.3). Fig. 15.3 Pictures showing the location of both the bursa with tendo Achilles tendon. ♦ There is a hypovascular zone 2 to 6 cm proximal to its insertion surrounded by thin paratenon, making it vulnerable to injuries and degeneration (Fig. 15.4). ♦ Talocalcaneal joint movements and hyperpronation increase this wringing effect. There are high stresses at the insertion. ♦ While running, the tendo Achilles tendon bears five to seven times of body weight ♦ Subtalar motion will produce rotational forces ♦ Malalignments of the foot and ankle will eccentrically load the tendon ♦ When the knee is straight and the ankle is dorsiflexed, there are high stresses at insertion ♦ Repetitive loads will lead to early tendon degeneration Diagnosis of rupture can be missed because of action of other active ankle flexors! ♦ Rupture can be at various sites, which are as follows: • High (musculotendinous junction)—9% • Midportion—72% • Calcaneal insertion—19% ♦ Predisposing factors leading to ruptures are as follows: • Preexisting tendinosis • Trauma • Leg muscle imbalance • Training errors • Pronation of foot • Use of steroids • Use of fluoroquinolones Diagnosis could be made easily if the answers to the following points are positive. ♦ History of “pop” or “snap” in the area ♦ Inability to bear weight ±. ♦ Palpable gap ♦ Positive Thompson’s test ♦ Repetitive tip toe raise may not be possible ♦ USG ♦ MRI Management of acute Achilles rupture is full of controversies! Box 15.1 lists the criteria for the selection of conservative and operative treatment. Box 15.1 Criteria for the selection of conservative and operative treatment. ♦ Conservative treatment: It is selected as per the following criteria: • Elderly patients • Sedentary patients • Diabetics • Smokers • Patients on steroids ♦ Operative treatment: It is selected as per the following criteria: • Young patients • Active patients • Sports population Tips and Tricks for Management of Tendo Achilles Ruptures ♦ Nonoperative care should be started as early as possible, within 48 hours of injury ♦ While doing nonoperative management, it is imperative to check preoperatively by USG that both the ruptured tendon ends meet with each other ♦ At conservative treatment, gradual reduction of plantarflexed position of ankle must be followed ♦ A midline incision may give a painful scar, while a lateral incision may damage the sural nerve; hence, a medial incision should be preferred ♦ At open repair, it is imperative not to create a plane between skin and tendon sheath ♦ Care of sural nerve is of utmost significance ♦ Continuous pull over tendon for 5 minutes will release the slackness and result in length gain up to 2 cm (Fig. 15.5) ♦ Put a pillow under the dorsum of foot while repairing the tendon to maintain the required plantarflexion ♦ Always drape both the legs at surgery for intraoperative comparison and accurate length restoration (Fig. 15.6) Fig. 15.6 Positioning at surgery showing a pillow under foot and draping of both the limbs. ♦ Avoid strangulating locking sutures as these may compromise tendon healing and may increase scarring ♦ Like repairs of flexor tendon in hand, reinforce repair with direct additional sutures ♦ Paratenon must be meticulously repaired for better healing process (Fig. 15.7)
15
Dealing with Tendo Achilles Problems!
Disorders of Tendo Achilles
Basic Science
Biomechanics
Acute and Chronic Tendo Achilles Rupture
Diagnosis
Management



Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


