15
Cubital Tunnel Syndrome
Eric Freeman, Dennis Rodin, and Kevin D. Plancher
History and Clinical Presentation
A 46-year-old right hand dominant man presented with numbness and tingling down the ulnar aspect of his left forearm and hand. Increased activities exacerbated his complaints. The patient reported that his symptoms were worse upon awakening in the morning. He had no impairment in his activities of daily living.
Physical Examination
There was no apparent forearm or hypothenar wasting of the left upper extremity. Range of motion of the elbow was measured as 0 to 125 degrees bilaterally. Areas were then examined for tenderness or ulnar nerve subluxation. There was tenderness with deep palpation over the cubital tunnel. Tinel’s test was negative at the cubital tunnel, carpal tunnel, and Guyon’s canal. The patient was examined for abduction of the small finger with extension (Wartenberg’s sign), which was negative. Earle’s test was negative (Fig. 15–1). Grip strength measured 60 pounds on the left and 65 pounds on the right. Intrinsic motor strength was 5/5 bilaterally, and there was no evidence of claw hand. On sensory examination, the patient had paresthesias in the fifth digit and ulnar aspect of the fourth digit. Two-point discrimination was greater than 10 mm in the fifth digit and ulnar aspect of the fourth digit, and less than 6 mm in the first, second, and third digits.
PEARLS
- The “no touch” technique when handling the ulnar nerve minimizes the risk of iatrogenic injury to the nerve itself as well as to its branches and blood supply.
- Avoid small incisions for adequate decompression.
PITFALLS
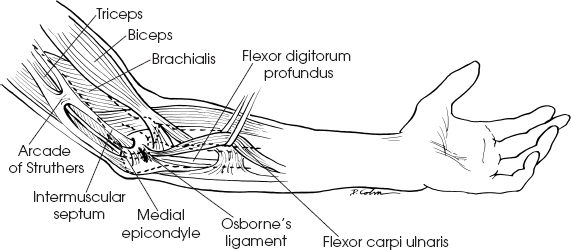
- Failure to release potential sites of compression proximally (i.e., the medial intermuscular septum and arcade of Struthers) may result in recurrence of symptoms despite adequate decompression of the cubital tunnel.
- Avoid injury to the MABC nerve to allow for normal sensation on posterior and inside ½ of elbow.
Diagnostic Studies
Anteroposterior and lateral radiographs of the left elbow showed no abnormalities. In patients with a history of trauma, a cubital tunnel projection radiograph can be performed to exclude osteophytes. Magnetic resonance imaging (MRI) can be helpful in the diagnosis, especially in patients who have undergone previous surgeries.
If the diagnosis of cubital tunnel syndrome is not certain, electromyography (EMG) may be helpful in determining the diagnosis and appropriate care.

Figure 15-1. Ability to cross the index and long fingers tests the ulna nerve (small muscles of the hand).
Differential Diagnoses
Cervical spine arthrosis
Cervical spine disk disease
Syringomyelia
Thoracic outlet syndrome
Pancoast tumor
Ulnar nerve entrapment in Guyon’s canal
Cubital tunnel syndrome
Diagnosis
Cubital Tunnel Syndrome
The patient was diagnosed with ulnar nerve compression at the level of the cubital tunnel. Cubital tunnel syndrome is now being diagnosed with increasing frequency. Our understanding of the dynamic nature of the pathophysiology has allowed us to improve its management. After an appropriate history and physical examination are performed, the diagnosis of ulnar nerve compression can be made. Following the diagnosis, it is crucial to determine the level of the lesion. In addition to a thorough physical examination, electrodiagnostic studies can be of great assistance in obtaining the definitive diagnosis. For this patient, electrodiagnostic studies were performed following 6 weeks of conservative treatment with no resolution of symptoms. EMG and nerve conduction studies revealed compression of the ulnar nerve at the level of the cubital tunnel in a sensory distribution.
The elbow flexion test is the most diagnostic test for cubital tunnel syndrome. The test involves the patient’s flexing the elbow past 90 degrees, supinating the forearm, and extending the wrist. Results are positive if discomfort is reproduced or paresthesia occurs within 60 seconds. The addition of shoulder abduction may enhance the diagnostic capacity of this test.
Nonsurgical Management
Conservative treatment of cubital tunnel syndrome is often successful with complete resolution of symptoms. Symptoms can be reduced by avoiding the activities that contribute to the nerve compression. This may include avoiding elbow flexion and resting on the elbow. In this case, the patient was placed in a long arm splint with the elbow flexed at 45 degrees. The splint was worn at night for 6 weeks. Activity modification was also attempted without relief of symptoms. Oral antiinflammatories may also be helpful in alleviating symptoms. When nonoperative modalities have failed over a period of 4 to 6 months, there are various surgical options.
Surgical Management
The patient was placed in the supine position on the operating table and the left upper extremity was prepped and draped in the usual sterile fashion. Intravenous antibiotics were given prophylactically. A sterile, well-padded tourniquet was then applied and inflated to 250 mm Hg following exsanguination. The intraoperative incision is marked out carefully to avoid injury to the median antebrachial cutaneous branch (Figs. 15–2 and 15–3). An incision was made on the medial surface of the elbow beginning 10 cm proximal to the epicondyle and extending distally ∼15 cm (Fig. 15–4). The subcutaneous tissue was sharply dissected until the two heads of the flexor carpi ulnaris were identified (Fig. 15–5). At this point, the arcuate ligament of Osborne may be visualized and divided, revealing the ulnar nerve in the cubital tunnel.