Congenital Overlapping Fifth Toe Deformity
Michael S. Downey
Jon M. Wilson Jr.
The congenital overlapping fifth toe deformity, also known as congenital digitus minimus varus or congenital digitus quinti varus, is a complex and challenging condition that requires equally complex and challenging treatment. There are three primary components to the overlapping fifth toe, which make it a triplane deformity. Adduction in the transverse plane, dorsiflexion in the sagittal plane, and varus rotation (i.e., external rotation) in the frontal plane all occur at the fifth metatarsophalangeal joint. Occasionally, contracture will also occur within the fifth toe itself. Due to the toe’s position, the deformity has shortening or contracture of the medial collateral ligament of the fifth metatarsophalangeal joint, the medial capsule of the fifth metatarsophalangeal joint, the extensor digitorum longus tendon slip of the fifth toe, and the skin of the dorsal fifth metatarsophalangeal joint and/or the dorsomedial aspect of the fourth interdigital web space. With time, osseous adaption of the proximal phalanx or fifth metatarsal head can also develop. Due to its position, the overlapping fifth toe will often appear smaller and flattened, losing its cylindrical appearance and taking on a paddle-like shape (Fig. 17.1). The deformity may be unilateral or bilateral and appears to occur equally in males and females (1).
ETIOLOGY
It is generally agreed that the overlapping fifth toe deformity is congenital and usually hereditary (Fig. 17.2). Several authors have attempted to explain the possible etiology. Lantzounis (2) felt that the deformity was secondary to a prolonged malposition of the fifth toe in utero. Others have suggested that the deformity may be secondary to the failure of the proper development of the articular surfaces of the fifth metatarsophalangeal joint. Dobbs (3) suggested that there might be a biomechanical role for the various components of the deformity. He described a displacement of the insertion of the flexor digitorum longus as the forefoot abducts on the rearfoot, especially in a pronated foot. This displacement leads to an abnormal medial force at the insertion of the long flexor into the distal phalanx. According to Dobbs, this leads to varus rotation of the fifth toe and adduction of the intermediate and distal phalanges. As the flexor tendon displaces, a stable plantarflexory force is lost, allowing dorsiflexory contracture at the fifth metatarsophalangeal joint. This biomechanical rationale may explain the deformity in some adults, or the progression of the deformity in some individuals, but does not appear to be the only etiology. As already noted, the deformity is often present at birth and clearly has developed before any weight-bearing force has been applied to the foot.
CLINICAL PRESENTATION
The congenital overlapping fifth toe deformity is usually asymptomatic in infancy and early childhood, but typically becomes symptomatic as the child matures and approaches adulthood. In some instances, the deformity does not become painful until later in life. Approximately 50% of overlapping fifth toe deformities remain asymptomatic throughout the patient’s life. Of those who develop symptoms, most will report dorsal digital irritation to the fifth toe or a painful heloma durum on the top of the toe. Conventional shoes often aggravate the toe. Less frequently, a heloma molle in the fourth web space or an onychoclavus (a corn or callous along the nail groove) will be the cause. Often, even when the deformity is asymptomatic, the patient or the parents may be concerned over the cosmetic appearance of the toe and the potential for future problems.
Careful evaluation of the overlapping fifth toe deformity will allow the clinician to determine its flexibility and the status of the fifth metatarsophalangeal joint. The tautness of the extensor digitorum longus tendon slip to the fifth toe and the dorsal-medial skin can be assessed by plantarflexing the fifth metatarsophalangeal joint. Palpation of the fifth metatarsophalangeal joint will generally allow estimation as to the amount of joint subluxation or dislocation. Radiographs will confirm the status of the fifth metatarsophalangeal joint and reveal any osseous adaption of the fifth ray components. Although not mentioned in the literature, the author has found that more aggressive treatment for the deformity is necessary if the deformity is more rigid in nature, associated with an irreducible or dislocated fifth metatarsophalangeal joint, or associated with congenital or adaptive osseous changes.
CONSERVATIVE TREATMENT
Most authors contend that conservative treatment is ineffective in the treatment of the congenital overlapping fifth toe deformity. In very mild cases or in the very young patient, stretching or strapping of the toe in abduction and plantarflexion can be attempted. Jordan and Caselli (4) advocated a simple adhesive splint, which they applied at as young an age as possible (but not younger than 4 or 5 months of age, because the digit is not long enough until then). They stated that “alignment of the deformed digits may be expected within 4 to 6 weeks depending upon the age of the patient and the severity of the deformity. Complete correction is then achieved by retaining the properly aligned digit for an additional 2 to 8 weeks in its corrected attitude” (4). In the older patient, accommodation is the only reliable nonsurgical treatment available. The use of padding, shields, or molds and extra-depth shoes or sandals may alleviate digital irritation in some patients.
 Figure 17.1 Classic appearance of congenital overlapping fifth toe deformity in an adult. Note the flattened or paddle-like appearance of the toe. |
When conservative treatment fails and/or when symptoms warrant, surgical intervention is indicated. Occasionally, a patient will request correction of an overlapping fifth toe deformity for cosmetic reasons alone and debate continues as to whether a surgeon should consider such a request. Those in favor of cosmetic correction suggest that most patients develop symptoms later in life and that early treatment of the deformity may help prevent later disability (5). Those against correction for cosmetic reasons alone argue that because approximately 50% of all cases remain asymptomatic, the risks of surgery do not merit the repair of the deformity when symptoms are not present. Hulman (6) reported good cosmetic results and patient satisfaction when a soft tissue repair of the deformity was performed primarily for cosmetic reasons. However, other authors have reported less than desirable results when operations for the correction of the overlapping fifth toe are performed primarily for cosmesis (7,8). Dyal et al (9) suggested that before performing surgery on a patient who is interested in improved cosmesis, the surgeon should consider showing the patient photographs of a typical postoperative result so that the patient has realistic expectations.
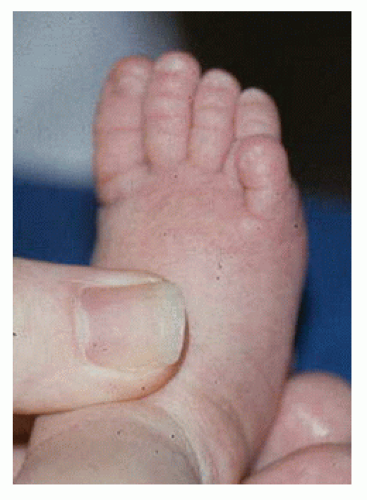 Figure 17.2 Congenital overlapping fifth toe deformity in a newborn. The presence of the deformity in a newborn strongly supports intrauterine or developmental factors as potential etiologies of the deformity. |
SURGICAL TREATMENT
Numerous procedures have been described in the literature for the correction of the congenital overlapping fifth toe deformity. The oldest surgery for the deformity is amputation. However, following simple amputation of the fifth toe, it became recognized that painful callouses developed around the head of the remaining fifth metatarsal (10). Other deformities, such as hammer toes, lesser digital drift, irritation to the fourth toe, or lesser metatarsalgia, have also frequently resulted after amputation (1) (Fig. 17.3).
In the 1940s, owing to the stigma associated with an amputation, and in some areas stimulated by the need for an alternative surgery in Civil Service applicants (who could not obtain Civil Service employment with either an overlapping fifth toe deformity or an amputated fifth toe), other procedures were developed. Most of these procedures emphasized soft tissue correction, but some also included osseous procedures. The objective of each technique was to reduce the three primary components of the deformity (the dorsiflexion, adduction, and varus rotation present at the fifth metatarsophalangeal joint).
In 1940, Lantzounis (2) described his proposed procedure. Through a dorsal longitudinal incision centered over the fifth metatarsophalangeal joint, he isolated the extensor digitorum longus tendon slip to the fifth toe and sectioned it at the distal end of the incision. He then longitudinally incised the periosteum over the distal end of the fifth metatarsal, the joint capsule, and the periosteum over the base of the proximal phalanx of the fifth toe. Lantzounis then created what he termed a “periosteocapsular flap” by elevating the incised periosteum and capsule dorsally, laterally, and medially. A drill hole was then created at the distal end of the fifth metatarsal, and the proximal end of the severed tendon slip was threaded through
the drill hole and sutured back onto itself. A horizontal mattress suture was placed into the “periosteocapsular flap” plantarly and tied with the toe held in a corrected position. Simply stated, the procedure was a modified Jones tenosuspension of the extensor digitorum longus tendon, a dorsal capsulotomy, and a plantar capsulorrhaphy. Lantzounis reported his results in 25 of the procedures in 19 patients. Patient ages ranged from 2 to 25 years old with an average age of 12 years old. One patient who had undergone correction for bilateral deformities was lost to follow-up, leaving a total of 23 operations that he reviewed from 8 months to 6 years postoperatively. Lantzounis found excellent results in 16 cases (70%), good results in 4 cases (17%), and poor results in 3 cases (13%).
the drill hole and sutured back onto itself. A horizontal mattress suture was placed into the “periosteocapsular flap” plantarly and tied with the toe held in a corrected position. Simply stated, the procedure was a modified Jones tenosuspension of the extensor digitorum longus tendon, a dorsal capsulotomy, and a plantar capsulorrhaphy. Lantzounis reported his results in 25 of the procedures in 19 patients. Patient ages ranged from 2 to 25 years old with an average age of 12 years old. One patient who had undergone correction for bilateral deformities was lost to follow-up, leaving a total of 23 operations that he reviewed from 8 months to 6 years postoperatively. Lantzounis found excellent results in 16 cases (70%), good results in 4 cases (17%), and poor results in 3 cases (13%).
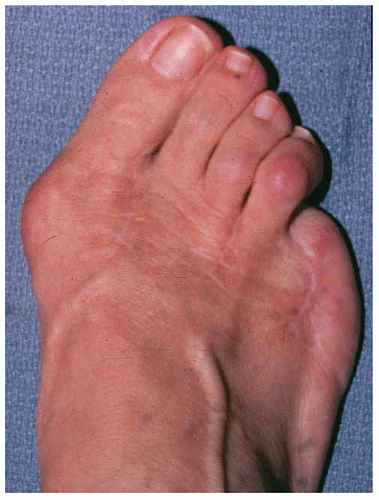 Figure 17.3 Patient who underwent amputation of a congenital overlapping fifth toe as a teenager. Note that the patient now has lateral drifting of her remaining lesser digits, a corn on the fourth toe, and a bunion deformity. The patient also complained of metatarsalgia under the fourth metatarsal. |
In 1942, Lapidus (11) described another unique procedure for the correction of the congenital overlapping fifth toe deformity. He approached the deformity through a hockeystick incision made along the dorsomedial border of the fifth toe, starting at the distal interphalangeal joint and running proximally to the fourth web space and then curving laterally over the dorsum of the fifth metatarsophalangeal joint and continuing dorsolaterally to the lateral aspect of the fifth metatarsal head. Next, a separate transverse incision was made over the extensor digitorum longus tendon at the midshaft of the fifth metatarsal. The extensor tendon slip to the fifth toe was identified and transected. The tendon was then gently pulled distally into the wound over the fifth toe. After the extensor tendon was harvested, a capsulotomy of the fifth metatarsophalangeal joint was performed. Next, an oblique subcutaneous channel was created from the distal interphalangeal joint of the fifth toe dorsomedially under the phalanges to the plantar-lateral aspect of the fifth metatarsophalangeal joint. The previously harvested extensor tendon was then rerouted through the channel created and sutured, under tension with the toe held in the corrected position, to the conjoined tendon of the abductor digiti quinti and flexor digitorum brevis to the fifth toe. Lapidus stated that his results had been “quite satisfactory” in a “few cases,” but did not give more specific details regarding the efficacy of his espoused procedure. De Palma and Zanoli (12) described a similar procedure, attributed to Zanoli who had earlier reported good, short-term results in four cases. De Palma and Zanoli (12) reported their results on 16 patients (7 bilateral, 23 feet total) with a mean age of 26 (range 19 to 40). Of the 18 feet available for follow-up, their mean time after operation was 8 years (range 4 to 17 years), and 10 (55%) were reported to show good correction, 5 (28%) were observed to be slightly overcorrected, and 3 (17%) were noted to be more severely overcorrected. No recurrences were observed and pain relief was noted in all their patients.
Whereas Lantzounis, Lapidus, and Zanoli primarily dealt with the extensor tendon and joint capsule, in 1943, Goodwin and Swisher (10) suggested release of the dorsal skin contracture as well. The authors advocated a Y-shaped incision over the dorsum of the fifth metatarsophalangeal joint with the stem of the Y extending proximally. The branches of the Y were situated diagonally distalward about halfway around the fifth toe. The incision was then carried deep, and a Z-plasty lengthening of the extensor digitorum longus tendon and a dorsal or dorsomedial capsulotomy of the fifth metatarsophalangeal joint was performed. The toe was held in the corrected position and closure was accomplished. The proximal arm of the Y is progressively closed distalward, allowing the triangular flap of skin to slip distally as far as is necessary to allow closure of the skin without tension. In this sense, the authors’ incision is closed in typical V-Y skin plasty fashion. Postoperatively, the authors stressed the need for maintenance of the corrected position for up to 6 weeks with either a plaster-of- Paris cast or an adhesive strapping. In reporting their results, the authors were brief in stating that their “technique has been highly successful in 100% of a series of about twenty cases, including males and females, children and adults, and patients in both private and institutional practice” (10).
Similar to Goodwin and Swisher, Stamm (13) and Wilson (14) described a V-Y skin plasty for part of the correction of the congenital overlapping fifth toe deformity. They created a V-shaped skin incision over the fourth web space with the base oriented distal-lateral and the apex proximal-medial. The skin flap was then elevated and a tenotomy of the extensor tendon and capsulotomy of the fifth metatarsophalangeal joint performed. Closure was then accomplished with the toe held in a corrected position and the incision closed in V-Y skin plasty fashion. Like Goodwin and Swisher, Wilson emphasized the need for postoperative maintenance of the correction with a plaster-of-Paris cast for several weeks. Wilson felt the procedure was best suited for patients under the age of 30 and reported his results in seven cases followed over a 2-year period. He described “very satisfactory” functional results in all of the cases, with one slight recurrence due to an error in operative technique. Stamm did not give any results in his description of the procedure.
Many years later, in 1990, Paton (15) reported on the longterm results of Stamm’s and Wilson’s approach. He noted that advocates of the V-Y plasty felt that the procedure was a successful, technically straightforward approach. Conversely, he noted that detractors of the operation insisted there was a high recurrence rate. Paton reviewed 20 V-Y plasty procedures in 16 children with a mean age of 9 years and 2 months. Early retrospective assessment of his cases demonstrated good results in 14 patients (70%), acceptable results in 3 patients (15%), and poor results in 3 patients (15%). Later follow-up at an average of 25 months postoperative revealed a marked deterioration in the reported success of the procedure. At the second follow-up, there were good results in 6 patients (30%), acceptable results in 2 patients (10%), and poor results in 12 patients (60%). In light of the poor long-term results, Paton recommended that the V-Y plasty approach for the correction of a congenital overlapping fifth toe deformity be abandoned.
In one of the most unique approaches, Cockin (16) reported on an operation he attributed to Mr. R. Weeden Butler. He related that Butler had performed his operation since the early 1950s. Cockin described Butler’s procedure as a double racquet incision with a circumferential incision around the toe (i.e., the racquet head) and a dorsal and plantar handle. The plantar handle was made slightly longer and was inclined laterally to allow improved position of the toe at closure. The skin flaps created were then raised with careful preservation of the neurovascular bundles. An extensor tenotomy and dorsal capsulotomy of the fifth metatarsophalangeal joint were performed. Next, the toe was swung downward and laterally into a corrected position and closure accomplished. After closure, the resultant dorsal incision would be longer than the plantar incision. Cockin reported on 70 cases in 55 patients (age range 5 months to 45 years). Follow-up evaluation was done from 1 to 10 years postoperative. Cockin reported 64 cases (91%) as having good results (i.e., satisfactory to both surgeon and patient with full
correction of the deformity), 4 cases (6%) as fair results (i.e., satisfactory to the patient with an element of the deformity left uncorrected), and 2 cases (3%) as failures (i.e., recurrence of the deformity). Cockin reported two cases of wound infection and three cases of delayed healing but no cases of long-term neurovascular compromise.
correction of the deformity), 4 cases (6%) as fair results (i.e., satisfactory to the patient with an element of the deformity left uncorrected), and 2 cases (3%) as failures (i.e., recurrence of the deformity). Cockin reported two cases of wound infection and three cases of delayed healing but no cases of long-term neurovascular compromise.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


