CHAPTER 30 Congenital Anomalies of the Cervical Spine
Basilar Impression
Basilar impression (or invagination) is a deformity of the bones of the base of the skull at the margin of the foramen magnum. The floor of the skull appears to be indented by the upper cervical spine, and the tip of the odontoid is more cephalad, sometimes protruding into the opening of the foramen magnum, and it may encroach on the brainstem. This deformity increases the risk of neurologic damage from injury, circulatory embarrassment, or impairment of cerebrospinal fluid flow. In 1939, Chamberlain1 first called attention to the clinical significance of this anomaly with the following vivid description:
There are two types of basilar impression: (1) primary, a congenital abnormality often associated with other vertebral defects, such as atlanto-occipital fusion, hypoplasia of the atlas, bifid posterior arch of the atlas, odontoid abnormalities, Klippel-Feil syndrome, and Goldenhar syndrome,2 and (2) secondary, a developmental condition usually attributed to softening of the osseous structures at the base of the skull, with the deformity developing later in life. Secondary basilar invagination is a potentially devastating sequelae of osteogenesis imperfecta, Hajdu-Cheney syndrome, and other osteochondrodysplasias.3 Although the precise etiology remains unclear, it has been suggested that the axial load from the cranium and its contents lead to recurrent microfractures in the region of the foramen magnum and precipitate flattening and infolding of the posterior skull base. This theory has been supported by intraoperative findings of thickened, proliferative callus at the skull base in patients with osteogenesis imperfecta.4,5 This thickened callus is also seen in conditions such as osteomalacia, rickets, Paget disease, renal osteodystrophy, rheumatoid arthritis, neurofibromatosis, and ankylosing spondylitis.6
Radiographic Features
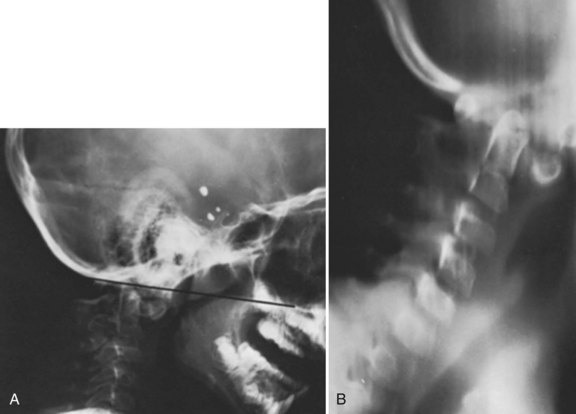
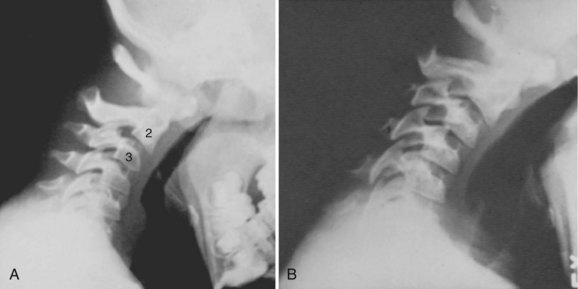
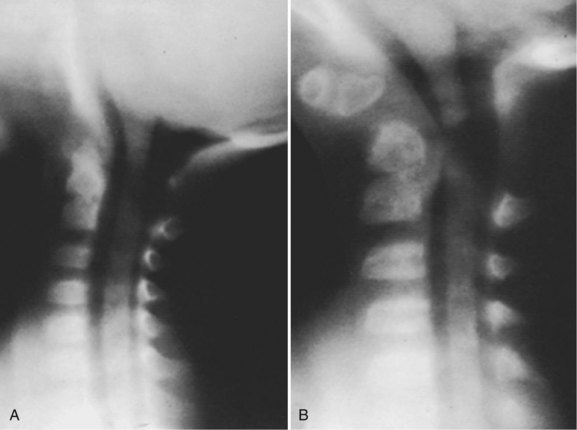
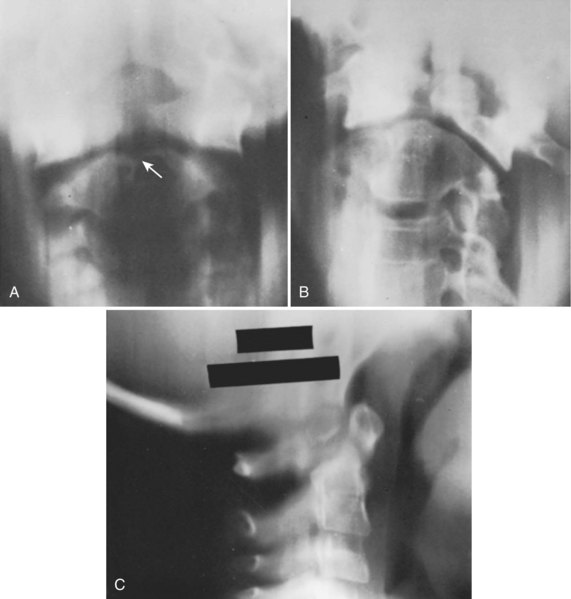
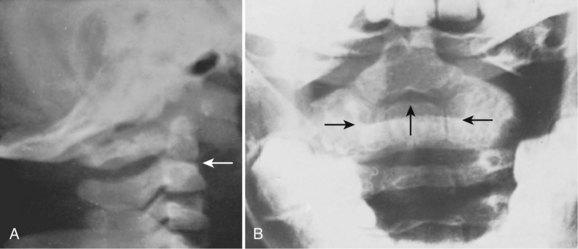
Basilar impression is difficult to assess radiographically. Many measurement schemes have been proposed; those most commonly referred to are the Chamberlain,1 McGregor,7 and McRae lines in the lateral radiograph (Fig. 30–1) and the Fischgold-Metzger line in the anteroposterior projection. The Chamberlain line1 (a line drawn from the dorsal marginal hard palate to the posterior lip of the foramen magnum) is seldom used because the posterior lip of the foramen magnum (opisthion) is difficult to define on a standard radiograph (Fig. 30–2A) and is often itself invaginated in basilar impressions.
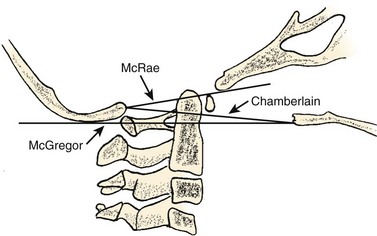
The McGregor line (a line drawn from the upper surface of the posterior edge of the hard palate to the most caudal point of the occipital curve of the skull) is easier to identify (see Figs. 30-1 and 30-2) and is preferable. The position of the tip of the odontoid is measured in relation to this baseline, and a distance of 4.5 mm above McGregor line is considered to be on the extreme edge of normality.7 The study of normal variations by Hinck and colleagues8 showed a wide range of normality, however, and difference between males and females.
A criticism of the lateral lines (McGregor and Chamberlain) is that the hard palate is not actually a part of the skull and may be distorted by an abnormal facial configuration or a highly arched palate, independent of a craniovertebral anomaly. In addition, the patient may have an abnormally long or short odontoid or an abnormality of the axis or occipital facets, which can diminish the value of the measurements. Upper cervical spine measurements on plain radiographs have an unacceptable interobserver reliability and intraobserver reproducibility. Although there are multiple factors for the wide variation between observers, many authors have suggested that the basion and opisthion are difficult to localize on radiographs and may be altered significantly by small changes in patient position.9
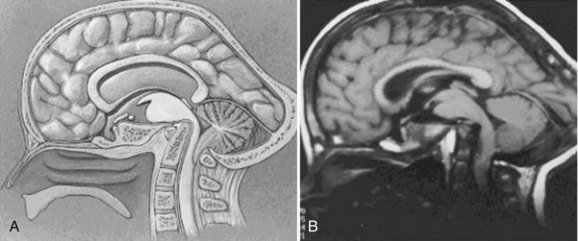
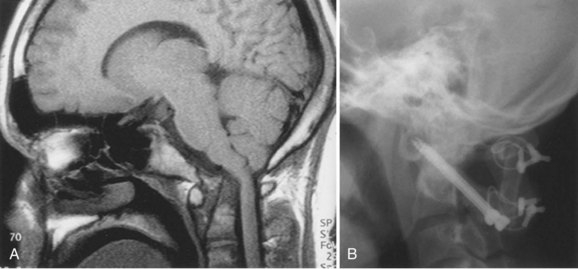
Since the advent of CT and MRI, the diagnosis of basilar invagination can be made directly rather than based on craniometric lines.10 These techniques have largely replaced the older tomography techniques, particularly the anteroposterior measurement of Fischgold and Metzger,10,11 which was previously the most accurate method. The mean and range of normal distances from the odontoid peg to the most frequently used skull baseline employing MRI was 1.2 mm (median 1.5 mm, SD 3 mm) below Chamberlain line; 0.9 mm (median 1.1, SD 3 mm) below McGregor line; and 4.6 mm (median 4.8, SD 2.6) below McRae line.10 MRI also allows direct assessment of the degree of neural compression and identifies the presence of associated pathologic processes, such as Chiari malformation, hydrocephalus, syringomyelia, or cerebellar herniation (Fig. 30–3).4 The lateral reference lines on plain radiographs are still very useful screening tools, however.12,13
Clinical Features
Patients with basilar impression frequently have a deformity of the skull or neck (e.g., a short neck in 78%, asymmetry of the face or skull or torticollis in 68%).14 These physical findings are often noted in patients without basilar impression (Klippel-Feil syndrome, occipitalization) and are not considered pathognomonic.
The symptoms (or lack of them) even in severe basilar impression are difficult to explain.13,14 The more segments involved in a patient with Klippel-Feil syndrome, the more likely it is that the odontoid will be superior.13 Basilar impression is frequently associated with anomalous neurologic conditions, such as Arnold-Chiari malformation14 and syringomyelia,15,16 which can cloud the clinical picture further. Symptoms are generally due to crowding of the neural structures at the level of the foramen magnum, particularly the medulla oblongata. The neurologic sequelae of basilar invagination are determined by the degree of cephalad migration of the clivus-atlas-dens complex. In addition to the direct compression of the ventral brainstem, the dens creates a fulcrum for traction on the cervical cord. Cerebellar dysfunction may arise from direct compression or reflect secondary herniation from the posterior fossa.
There is an unusually high incidence of basilar impression in northeast Brazil,17 and the work of De Barros and colleagues14 has been helpful in delineating the symptoms and signs. Patients who were symptomatic with pure basilar impression had the dominant complaints of motor and sensory disturbances, and 85% had weakness and paresthesia of the limbs. In contrast, patients who were symptomatic with pure Chiari malformation were more likely to have cerebellar and vestibular disturbances (unsteadiness of gait, dizziness, and nystagmus). In both conditions, there may be impingement of the lower cranial nerves as they emerge from the medulla oblongata, particularly the trigeminal (V), glossopharyngeal (IX), vagus (X), and hypoglossal (XII) nerves.14 Headache and pain in the nape of the neck, in the distribution of the greater occipital nerve, are common findings.14,18
Posterior encroachment may cause blockage of the aqueduct of Sylvius, and the presenting symptoms may be from increased intracranial pressure or hydrocephalus.7,14 Compression of the cerebellum with vestibular involvement or herniation of the cerebellar tonsils (Chiari malformation) is a frequent finding,14 leading to vertical or lateral nystagmus in 65% of cases. These symptoms may be caused not by direct pressure from the posterior rim of the foramen magnum but rather by a thickened band of dura invisible on plain radiographs; this has prompted several authors to recommend routine MRI evaluation. If this situation is unrecognized, bony decompression alone (without opening the dura) would be unsuccessful in obtaining remission of symptoms or halting progression of the neurologic injury.14
There is a high incidence of vertebral artery anomalies in basilar impression, atlanto-occipital fusion, and absence of the C1 facet.19 In addition, the vertebral arteries may be compressed as they pass through the crowded foramen magnum, causing symptoms suggestive of vertebral artery insufficiency, such as dizziness, seizures, mental deterioration, and syncope.7,19,20 These symptoms may occur alone or in combination with symptoms of spinal cord compression.7,14,19,21 Michie and Clark22 and Bachs and colleagues23 theorized that one explanation for the frequent association of syringomyelia or syringobulbia and basilar impression is that the vertebral arteries and the anterior spinal artery are compromised in the region of the foramen magnum, with subsequent degeneration of the spinal cord and medulla. Arteriographic studies are unavailable to confirm this thesis. Children with occipitocervical anomalies may be more susceptible to vertebral artery injury and brainstem ischemia, particularly children who undergo skull traction for correction of scoliosis. Moderate amounts of traction (<15 lb) that normally would be well tolerated may compromise these abnormal vessels. Careful radiographic evaluation of the occipitocervical junction should precede any use of skull traction, even if only minimal traction forces are planned.24
Although this condition is congenital, many patients do not develop symptoms until the 2nd or 3rd decade of life.13,14 These delayed symptoms may be due to a gradually increasing instability from ligamentous laxity caused by aging, similar to the delayed myelopathies reported after atlantoaxial dislocations or the increasing instability of C1 and C2 in patients with odontoid agenesis.25 These individuals often develop premature cervical osteoarthritis, as found in the family studies of Gunderson and colleagues.21 Chamberlain1 and others theorized that the young developing brain may be more tolerant of compressive effects, which later prove deleterious to older tissues. Similarly, arteriosclerotic changes in the vertebral arteries may make these vessels more susceptible to minor constrictions. Symptoms frequently occur in older patients in whom a congenital anomaly would not ordinarily be considered. Patients with this malformation have been mistakenly diagnosed as having multiple sclerosis, posterior fossa tumors, amyotrophic lateral sclerosis, or traumatic injury. It is important to survey this area whenever such a diagnosis is considered and whenever this malformation is suspected.
Treatment
Treatment depends on the cause of the symptoms and often requires the teamwork of an orthopaedist, neurosurgeon, neurologist, and radiologist. It is possible to have a severe basilar impression without neurologic symptoms, and a search for associated conditions must be conducted. Hydrocephalus from aqueductal stenosis, if present, must be addressed first with ventricular shunting before any other surgical interventions.4
Treatment of symptomatic basilar invagination is dictated by the severity of ventral neural compression and reducibility of the deformity. An initial attempt should be made to realign the cervical spine and decompress the neural elements by head positioning and, in some cases, halo traction. Plain radiographs and MRI may be used to determine the adequacy of reduction and neural decompression. Patients who respond to such closed reduction methods may be treated with suboccipital craniectomy and upper cervical laminectomy, followed by occipitocervical arthrodesis. More recent reports suggest that many of the physical changes can be reversed by atlantoaxial distraction fixation surgery.26,27 Most authors suggest opening the dura to look for a tight posterior dural band.14 Brainstem compression not relieved by traction demands anterior decompression and resection of the offending anterior atlas, odontoid, or distal clivus. Posterior decompression and fusion are also necessary and may be performed immediately after or as a staged procedure.28
Posterior fossa decompression alone for symptomatic secondary basilar invagination typically provides only transient relief of symptoms, followed by recurrent neurologic deterioration months to years after the index procedure. Studies have shown that secondary basilar invagination in patients with osteochondrodysplasia tends to progress even after occipitocervical fusion with infolding of the skull base around the fusion mass and progressive forward bending.3 Prolonged bracing with an orthotic device and lifelong surveillance may be prudent to halt further recurrence or symptomatic progression.4 These recommendations are generalizations regarding treatment, and appropriate references should be consulted in the evaluation of individual patients.
Atlantoaxial Instability
The clinical significance of a bony anomaly in the region of the atlantoaxial joint is primarily related to its influence on the stability of this articulation. The precipitating factor may be an abnormal odontoid, atlanto-occipital fusion, or laxity of the transverse atlantal ligament, but the end result is narrowing of the spinal canal (encroachment) and impingement on the neural elements.29 It is important not to lose sight of this basic problem, but frequently it becomes obscured in radiographic detail, conflicting reports, and unusual clinical symptoms and signs. It is important to review atlantoaxial instability before a detailed discussion of the individual anomalies that may be contributory.
Pathomechanics
The articulation between C1 and C2 is the most mobile part of the vertebral column and normally has the least stability of any of the vertebral articulations. The normal cervical spine permits about 90 degrees of rotatory motion; 50% of this motion occurs in the atlantoaxial joint. Considerable shifting from side to side (lateral slide) also occurs as a component of this rotatory motion. Flexion and extension are permitted to a limited degree (normally about 10 degrees of extension and 5 degrees of forward flexion); more than 10 degrees of flexion indicates subluxation.30 The odontoid acts as a bony buttress to prevent hyperextension, but the remaining normal range of motion is maintained and is solely dependent on the integrity of the surrounding ligaments and capsular structures.
Motion of the atlantoaxial articulation is usually accentuated in patients with bony anomalies of the occipitocervical junction. An excellent example is a patient with atlanto-occipital fusion, who is frequently found to have compensatory hypermobility of the atlantoaxial joint. If this same patient has an associated synostosis of C2-3, it is reasonable to expect that this additional stress on the atlantoaxial articulation may eventually lead to significant instability.28,29,31,32 This assumption has clinical support in that 60% of patients with symptomatic atlanto-occipital fusion have associated fusion of C2-3.29,32,33
More likely, the degenerative changes of aging cause the lower cervical articulations to become more rigid. This gradual restriction of motion below places an increased demand on the ligaments and capsular structures of the atlantoaxial articulation, with the development of instability.34 With aging, the central nervous system itself becomes less tolerant of intermittent compression, and its ability to recover is diminished. There is evidence to suggest that intermittent compression is more harmful or irritating to the spinal cord than static, constant compression.35 Arteriosclerosis and loss of elasticity from aging affect the vertebral arteries, making them more sensitive to compression at the foramen magnum.36
In patients with basilar impression or atlanto-occipital fusion, the clinical findings suggest that the major damage is occurring anteriorly from the odontoid. The symptoms and signs of pyramidal tract irritation, muscle weakness and wasting, ataxia, spasticity, hyperreflexia, and pathologic reflexes are commonly found.33,37 Autopsy findings consistently show that the brainstem is indented by the abnormal odontoid.37,38 Other, less common complaints include diplegia, tinnitus, earaches, dysphasia, and poor phonation, all of which are due to cranial nerve or bulbar irritation from direct pressure of the odontoid on the medulla.
If the primary area of impingement is posterior from the rim of the foramen magnum, the dural band, or the posterior ring of the atlas (typical of odontoid anomalies), symptoms are referable to the posterior columns with alterations in deep pain and vibratory responses and proprioception. If there is also an associated cerebellar herniation, nystagmus, ataxia, and incoordination may be observed. Symptoms referable to vertebral artery compression—dizziness, seizures, mental deterioration, and syncope—may occur alone or in combination with symptoms of spinal cord compression.34
In children, the presenting symptoms may be quite subtle and nonspecific. Perovic and colleagues39 reported that in most of their patients the only presenting symptom was generalized weakness, manifested as lack of physical endurance, a history of frequent falling, or the child’s asking to be carried. Pyramidal tract signs appeared later, and posterior column signs and sphincter disturbances were less frequently encountered.39 Similarly, in achondroplasia, retardation of motor skills and increasing hydrocephalus may be the only clinical manifestation of impending quadriparesis secondary to basilar stenosis.
Atlantoaxial Instability and Down Syndrome
Spitzer and colleagues40 were the first to describe occipitoatlantal instability and atlantal hypoplasia in Down syndrome. Generalized ligamentous laxity and flat facets predispose to hypermobility and pathologic motion at the craniovertebral and atlantoaxial articulations. Depending on patient age at the time of the study, 10% to 40% of these patients have radiologically detectable atlantoaxial instability.40,41
The natural history of atlantoaxial instability in patients with Down syndrome is not well known. Burke and colleagues42 reported 7 of 32 patients developing atlantoaxial instability over a 13-year period. Morton and colleagues43 found no evidence of de novo atlantoaxial instability in 67 patients with Down syndrome over a 5-year period. In addition, a direct correlation between neurologic deterioration and atlantoaxial instability has not been established. Ferguson and colleagues44 identified 17 of 84 patients with atlantoaxial instability on plain radiographs but could not correlate any difference in neurologic symptoms with radiographic findings. Taggard and colleagues45 did not find such a benign relationship between C1-2 instability and neurologic function, however, reporting acute neurologic deterioration in six patients after a minor fall or intubation for a general anesthetic.
Radiographic Features
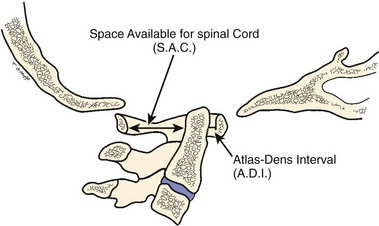
The atlas-dens interval (ADI) is the space seen on the lateral radiograph between the anterior aspect of the dens and the posterior aspect of the anterior ring of the atlas (Fig. 30–4). In children, the ADI should be no greater than 4 mm,30 particularly in flexion, where the greatest distance can be noted. The upper limit of normal in adults is less than 3 mm. Occasionally, the space between the odontoid and the ring of C1 forms a “V” shape in flexion; in this situation, the ADI is measured at the mid-portion of the odontoid. A subtle increase in the ADI in the neutral position may indicate disruption of the transverse atlantal ligament. The ADI is a valuable aid in the evaluation of acute injury, when standard flexion-extension views would be potentially hazardous.30,46 Fielding and colleagues47 noted that the shift of C1-2 does not exceed 3 mm in adults if the transverse ligament is intact. The transverse ligament ruptures within the range of 5 mm.48 Similar data for children are unavailable.
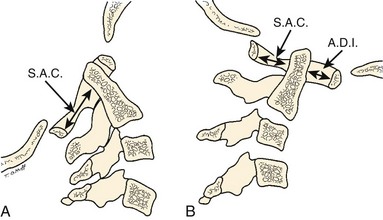
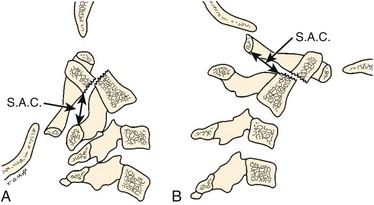
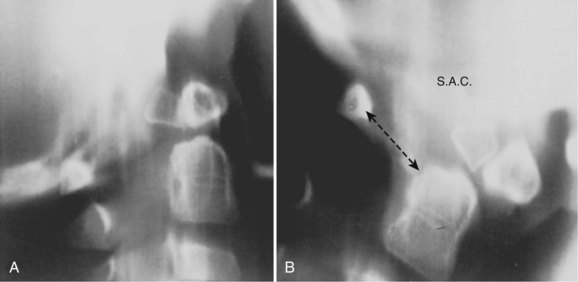
The ADI is of limited value in evaluating chronic atlantoaxial instability owing to congenital anomalies, rheumatoid arthritis, or Down syndrome. In these conditions, the odontoid is frequently found to be hypermobile with a widened ADI, particularly in flexion (Fig. 30–5), but not all are symptomatic, and all do not require surgical stabilization.42,48 In this situation, attention should be directed to the amount of space available for the spinal cord (SAC). Determining the SAC is accomplished by measuring the distance from the posterior aspect of the odontoid or axis to the nearest posterior structure (foramen magnum or posterior ring of the atlas).29,32,49 This measurement is particularly helpful in evaluating a patient with nonunion of the odontoid or os odontoideum because in both conditions the ADI may be normal, yet in flexion or extension there may be considerable reduction in the space available for the spinal cord (Fig. 30–6).50 Lateral flexion-extension views should be conducted voluntarily by the patient, particularly a patient with a neurologic deficit (Fig. 30–7). Most symptomatic patients exhibit significant instability.
Patients with a normal odontoid process and an attenuated or ruptured transverse atlantal ligament are particularly at risk; with anterior shift of the atlas over the axis, the spinal cord is easily damaged by direct impingement against the intact odontoid process,50,51 such as in atlanto-occipital fusion. The situation is less dangerous if the odontoid process is absent or fractured and is carried forward with the atlas (os odontoideum).47 In a large series of patients with os odontoideum reported by Fielding and colleagues,47 the average displacement was 1 cm, mostly either anterior or posterior, but some were unstable in all directions.
In patients with multiple anomalies, the usual radiographic views are not always reliable in confirming the presence or absence of an odontoid.39 Similarly, in patients with abnormal bone, such as patients with Morquio syndrome or spondyloepiphyseal dysplasia, the odontoid may be present but dysplastic, blending with the surrounding abnormal bone, and cannot be differentiated. In these situations, adequate visualization can be obtained by using lateral laminagraphic techniques (see Fig. 30–2) or with a CT scan with reconstruction views.52,53 When the exact cut at the level of the odontoid is determined, it is repeated in flexion-extension to ascertain the stability of the atlantoaxial articulation. Extension views should not be ignored. Many patients have been found to have significant posterior subluxation.29,47,54 Dynamic (flexion-extension) CT scans have been used to show this area, particularly with lateral reconstruction, and have replaced the laminagraphs.51–53
Dynamic MRI provides direct vision of the neurologic structures and in many cases the site of bony impingement and cord compression that may not be appreciated on routine views.52,55–57 CT scans have been extremely helpful in evaluating anomalies of the upper cervical spine. Three-dimensional reconstruction aids in visualizing anatomic relationships. Dynamic CT or MRI flexion and extension views are difficult to perform and time-consuming, but they can provide graphic evidence of looseness.58 MRI similarly has been helpful in showing the relationship of the neurologic structures to the bony anatomy, such as the Chiari malformation and syringomyelia.55,58 Also, the transverse atlantal ligament can be visualized with MRI.55
Steel59 called attention to the checkrein effect of the alar ligaments and how they form the second line of defense after disruption of the transverse atlantal ligament (Fig. 30–8). This secondary stability no doubt plays an important role in patients with chronic atlantoaxial instability.60 Steel’s anatomic studies provided a simple rule that is helpful to physicians evaluating this area. He defined the “rule of thirds”: The area of the vertebral canal at C1 can be divided into one third odontoid; one third spinal cord; and one third “space,” which represents a safe zone in which displacement can occur without neurologic impingement and is roughly equivalent to the transverse diameter of the odontoid (usually 1 cm).59
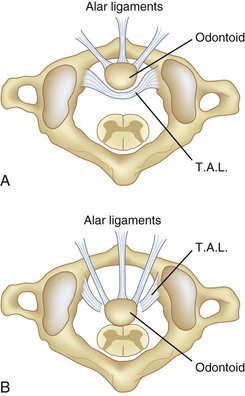
In chronic atlantoaxial instability, it is of prime importance to recognize when the patient has exceeded the “safe zone” of Steel and enters the area of impending spinal cord compression. At this point, the second line of defense, the alar ligaments, has failed, and there is no longer a margin of safety (see Fig. 30–8).48 Experimentally, Fielding and colleagues48 found that after rupture of the transverse ligament, the alar ligaments are usually inadequate to prevent further displacement of C1-2 when a force similar to that which ruptured the transverse ligament is applied. Although the alar ligaments appear thick and strong, they stretch with relative ease and permit significant displacement.
McRae33 was first to call attention to the relationship of neurologic symptoms and the sagittal diameter of the spinal canal (SAC) (see Fig. 30–4). He noted that his patients with atlanto-occipital fusion with less than 10 mm of available space behind the odontoid or atlas were always symptomatic. With the availability of more clinical data, this measurement has been more specifically defined. After an extensive review of the literature, Greenberg34 determined that in adults spinal cord compression always occurs if the sagittal diameter of the cervical canal behind the dens is 14 mm or less. Cord compression is possible between 15 mm and 17 mm and never occurs if the distance is 18 mm or more. Variations in patient size and the presence or absence of soft tissue elements affect the clinical significance of the measurement, however. Jauregui and colleagues56 refined these measurements further for children. MRI may be helpful in assessing the integrity of the transverse atlantal ligament.55 In some patients, myelography has shown a ventral impingement secondary to a thick wad of radiolucent soft tissue posterior to the dysplastic odontoid and the body of the axis.39
Data on normal variations in sagittal and transverse diameter of the cervical spine have been collected for infants, children, and young adults.46,61,62 As might be expected, these measurements generally are smaller than in adults and follow a predictable growth curve. Clinical significance is determined via two parameters: (1) comparison of the absolute diameter with the known norms for that vertebral level and age, and (2) comparison of successive vertebral levels within the same individual. Variations in the latter are more sensitive in determining an abnormality involving a single vertebra because there is good correlation between adjacent levels in the same child. These measurements should be readily available when evaluating the growing spine for pathologic narrowing and expansion.63 The transparencies developed by Haworth and Keillor61 are particularly helpful in this regard and provide an efficient screening test for assessing the transverse diameter of the spinal canal in the growing child. The sagittal diameter of the cervical canal is largest at C1 and gradually narrows in size until C5-7. The appearance is similar to a funnel, and enlargement in the outline suggests an intraspinal mass, even if the absolute measurements do not exceed the upper limits of normal.63
In children, there are several normal variations in cervical spine mobility that can be alarming to physicians who are unaware of them. Cattell and Filtzer64 called attention to the frequent (20%) finding of overriding of the anterior arch of the atlas on the odontoid with extension of the neck. This variation is due to normal elasticity of ligaments and diminishes with growth; it is not present after age 7 years. Pseudosubluxation of 3 mm of C2 on C3 can be found in more than one half of children younger than age 8 years (Fig. 30–9).64–66 Swischuk66 suggested a posterior cervical line that is useful in differentiating physiologic from pathologic anterior displacement of C2 on C3. Less frequently, hypermobility occurs at the C3-4 interspace. Recognition becomes particularly important when evaluating a young child who has Klippel-Feil syndrome or has undergone recent trauma.
The normal pattern of ossification of the cervical spine in children can pose problems in radiographic interpretation. At birth, the odontoid is separated from the body of the axis by a wide cartilaginous band, which represents the vestigial disc space, referred to as the neurocentral synchondrosis (see section on anomalies of odontoid). On the lateral radiograph, this lucent line is similar in appearance to an epiphyseal growth plate. This line may be confused with the jointlike articulation between the odontoid and the body of the atlas found in os odontoideum; this is present in nearly all children at age 3 and absent in most by age 6. Consequently, the diagnosis of os odontoideum in children must be confirmed by showing motion between the odontoid and the body of the axis. Atlantoaxial fusion may be difficult to diagnose in a young child because a significant portion of the ring of C1 is unossified at birth. There is usually a 5- to 9-mm gap posteriorly, which ossifies by age 4.31 The anterior arch of the atlas is invisible in 80% of infants, and the entire ring may not be completely ossified until age 10 years.31,53
Myelography can be helpful in defining an area of constriction. In this regard, gas or water-soluble contrast agent (metrizamide) myelography should be used in preference to myelography with oil contrast media (Fig. 30–10).33,39,67,68 CT in conjunction with metrizamide myelography is particularly helpful in evaluating children with rotational deformities or compromise of the neural canal in the upper cervical spine.51,67,68
MRI allows a more complete and accurate examination of the soft tissues and brainstem and assists in identifying the area of direct impingement in individuals with occipitocervical anomalies.57 Dynamic flexion-extension MRI allows for improved selection of patients for cervical arthrodesis and allows direct determination of the need for concurrent anterior or posterior decompression of neural elements.52,58 Surgical stabilization may be avoided or delayed in individuals with mild radiographic instability without spinal cord compromise.
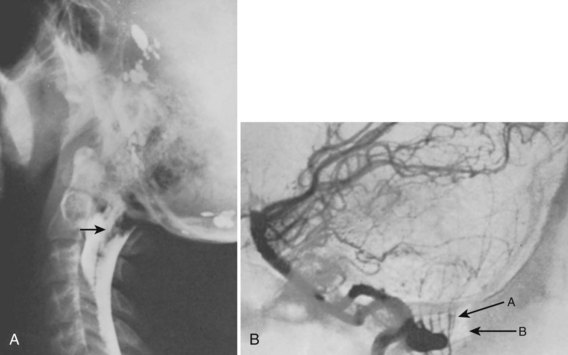
Excessive motion at the occiput-C1 may lead to compression of the vertebral arteries.53 Vertebral arteriography is helpful in evaluating patients who exhibit symptoms of transient brainstem ischemia.24,69,70 If cerebellar herniation (Chiari malformation) is suspected, arteriography combined with myelography can show the anomaly (Fig. 30–11).68
Treatment
Effective treatment generally can be provided only if the exact cause of symptoms has been determined by a careful correlation of the clinical and radiologic findings. Before surgical intervention, reduction of the atlantoaxial articulation should be achieved by either positioning or traction.28,60,65,71 Operative reduction should be avoided, if possible, because it is associated with increased morbidity and mortality rates.72,73 The patient should be maintained in the reduced position preoperatively until spinal cord edema and local irritation resolve; this is usually accompanied by improvement of the neurologic status and often remission of symptoms. If neurologic symptoms are unchanged with reduction and rest, the physician should carefully seek other causes.
Various techniques for surgical stabilization of atlantoaxial instability have been used in pediatric patients with good results.60,74 Sublaminar wiring, C1-2 transarticular screws, transoral decompression with posterior plating, and laminectomy with Steinmann pin occipitocervical fusion all have been reported with good results (Fig. 30–12).28,45 Choice of surgical procedure for stabilization must be individualized based on clinical presentation and surgeon expertise.28,71

Too little attention has been paid in the past to occult respiratory dysfunction in patients with atlantoaxial instability.74,75 Many patients have an unrecognized decrease in vital capacity and chronic alveolar hypoventilation as a result of the neurologic injury to the brainstem.18,76 Similarly, gag and cough reflexes are often depressed,74 and the patient may experience a deterioration of pulmonary function in the postoperative period.76 Periods of apnea and respiratory distress during surgery or in the immediate postoperative period have frequently resulted in death or have required prolonged respiratory support.76 Preoperative pulmonary evaluation can be helpful in limiting the severity of respiratory complications. If pulmonary function is significantly reduced or if gag and cough reflexes are depressed, consideration should be given to preoperative tracheostomy.74 Equipment for mechanical respiratory support must be immediately available during the postoperative period.76
Laxity of Transverse Atlantal Ligament
Laxity of the transverse atlantal ligament is a diagnosis of exclusion suggested by the clinical occurrence of chronic atlantoaxial dislocation without a predisposing cause.33 There is no history of trauma, congenital anomaly, infection, or rheumatoid arthritis to account for the radiologic finding. Most patients with this condition have the typical symptoms of atlantoaxial instability and require surgical stabilization.
Laxity of the transverse atlantal ligament is unusually common in patients with Down syndrome, with a reported incidence of 15% (Fig. 30–13).42,77 The lesion may be found in all age groups, with no age preponderance.42 These patients seem to have rupture or attenuation of the transverse atlantal ligament with encroachment of the safe zone of Steel (see Fig. 30–8), but at least initially they are protected by the checkrein action of the alar ligaments from spinal cord compression (see Fig. 30–13). In other words, many patients have excessive motion, but relatively few are symptomatic, and most cases are discovered only by radiologic survey.78 If radiographs of the upper cervical spine indicate an ADI of more than 5 mm, instability is considered to be present. Usually, if symptoms are present, instability of greater than 7 to 10 mm is found. MRI can be helpful in assessing the integrity of the transverse atlantal ligament.55
Complete data are unavailable regarding the best way to manage this problem.42,77,78 Very little is known about the natural history, despite radiographic examination of hundreds of children.78 Studies have indicated that some children experience progressive looseness with time; others who manifest small degrees of instability can occasionally become stable.42 Currently, radiographic examination on a routine basis is recommended for children with Down syndrome, particularly children who compete in athletics.77 Any child with Down syndrome who has a musculoskeletal complaint, such as subluxing patella, dislocating hips, or unsteady gait, should be investigated. In addition, evaluation of the cervical spine should be a part of the preoperative assessment in these cases.
A patient with Down syndrome and no evidence of radiographic instability requires no activity restrictions other than avoidance of collision sports.42–44 With current knowledge, prophylactic stabilization is not indicated. When a patient develops atlantoaxial instability and is neurologically intact, any sport with the potential to stress the cervical spine should be avoided. The Special Olympics has identified gymnastics, high jump, diving, butterfly and breast stroke swimming, and pentathlon to be at-risk activities.42 The use of a cervical collar in these patients is controversial. Progressive instability, neurologic symptoms, or both are indications for surgical stabilization.34,42
Occipitoatlantal Instability
Occipitoatlantal instability is a rare condition often caused by trauma or, less commonly, congenital abnormalities.79,80 Previously, most patients did not survive this injury, but with improved resuscitative measures, the problem has been reported more frequently. Clinical and neurologic manifestations include cardiorespiratory arrest, motor weakness, quadriplegia, torticollis, pain in the neck, vertigo, and projectile vomiting.79 Surgical stabilization is usually necessary. Anomalies of the upper cervical spine can also lead to this condition, and it has been reported in association with Down syndrome. The curvature of the occipital condyle in healthy children increases by 60% from infancy to adolescence.80 Patients who have Down syndrome and occipitoatlantal instability fail to develop this curved architecture in the occipital condyle.80
Atlanto-occipital Fusion (Occipitalization, Occipitocervical Synostosis, Assimilation of Atlas)
Atlanto-occipital fusion is characterized by a partial or complete congenital union between the atlas and the base of the occiput (Fig. 30–14). It ranges from total incorporation of the atlas into the occipital bone to a bony or fibrous band uniting one small area of the atlas to the occiput.81 Basilar impression is commonly associated with occipitocervical synostosis; other associated anomalies include Klippel-Feil syndrome, occipital vertebrae, and condylar hypoplasia.31,32
Occipitocervical synostosis, basilar impression, and odontoid anomalies are the most common developmental malformations of the occipitocervical junction. Incidence ranges from 1.4 to 2.5 per 1000 children.31,82 Gholve and colleagues32 found a predominance in boys of 80%.
Clinical Features
Most patients have an appearance similar to that in Klippel-Feil syndrome, with a short, broad neck; a low hairline; torticollis; a high scapula; and restricted neck movements.35,37,83 The skull may be deformed and shaped like a “tower.” Kyphosis and scoliosis are frequent. Other associated anomalies occasionally seen include dwarfism, funnel chest, pes cavus, syndactylies, jaw anomalies, cleft palate, congenital ear deformities, hypospadias, and sometimes genitourinary tract defects.
Neurologic symptoms do not usually occur until the 3rd or 4th decade but can manifest during childhood.32,84 Symptoms progress in a slow, unrelenting manner and may be initiated by traumatic or inflammatory processes. Symptoms rarely begin dramatically, but they have been reported as a cause of sudden death.85 It is difficult to explain why neurologic problems develop so late and progress so slowly in these patients. It may be that the frequently associated atlantoaxial instability progresses with age and the resultant added demands placed on this articulation, producing gradual spinal cord or vertebral artery compromise.
McRae and Barnum83 suggested that the key to development of neurologic manifestations lies with the odontoid and its position, an indication of the degree of actual or relative basilar impression. If the odontoid lies below the foramen magnum, the patient is usually asymptomatic.33 With the decrease in vertical height of the atlas, the odontoid may project well into the foramen magnum, producing brainstem pressure, a fact well documented by autopsy.37,38
Anterior compression of the brainstem from the backward-projecting odontoid is most common (see Fig. 30–14). This compression produces various findings, depending on the location and the degree of pressure. Pyramidal tract signs and symptoms (spasticity, hyperreflexia, muscle weakness and wasting, and gait disturbances) are most common, but cranial nerve involvement (diplopia, tinnitus, dysphagia, and auditory disturbances) may be seen less often. Compression from the posterior lip of the foramen magnum or the constricting band of dura may disturb the posterior columns, resulting in loss of proprioception, vibration, and tactile discrimination. Nystagmus, a common occurrence, is probably due to posterior cerebellar compression.
Vascular disturbances from vertebral artery involvement may occasionally result in syncope, seizures, vertigo, and unsteady gait, among other signs and symptoms of brainstem ischemia.15,53 Disturbed mechanics of the cervical spine may result in a dull aching pain in the posterior occiput and neck with episodic neck stiffness and torticollis.15 Tenderness noted in the area of the posterior scalp may be due to irritation of the greater occipital nerve. The following most common signs and symptoms occur, in decreasing order of frequency: pain in the occiput and neck, vertigo, unsteady gait, paresis of the limbs, paresthesias, speech disturbances, hoarseness, double vision, syncope, auditory noise or disturbance, and interference with swallowing. Acute respiratory failure secondary to hypoventilation and sleep apnea may occur.15 All these may be manifestations of underlying atlantoaxial instability, which, as an isolated lesion, may produce neck pain, headaches, and neurologic deficits from cord or root irritation and, rarely, sudden death.34,73
Radiographic Features
Standard radiographs of this area can be difficult to interpret. Tomography, CT, and MRI may be necessary to clarify the pathologic condition (see Fig. 30–14).15,52,53,84,85 Most commonly, the anterior arch of the atlas is assimilated into the occiput, usually in association with a hypoplastic posterior arch. The condition may range from total incorporation of the atlas into the occipital bone to a bony or fibrous band uniting one small area of the atlas to the occiput. CT scans are often necessary to show bony continuity of the anterior arch of the atlas with the occiput. Posterior fusion is not usually evident because this portion of the ring may be represented only by a short bony fringe on the edge of the foramen magnum. Despite its innocuous radiologic appearance, this fringe is frequently directed downward and inward, can compromise the spinal canal posteriorly, and has been found to create a groove in the spinal cord. It is usually assumed that the assimilated atlas is fused symmetrically to the occipital opening, but several autopsy specimens have shown a posterior positioning of the atlas.83 This position, in effect, pushes the odontoid posteriorly, narrowing the spinal canal and the space available for the spinal cord.
Ossification of the atlas proceeds from paired centers—one for each of the lateral masses. These progress posteriorly into the neural arches, which are fully ossified at birth except for a gap of 5 to 9 mm posteriorly that closes by the 4th year.53 The anterior arch of the atlas is invisible in 80% of neonates. This area most commonly ossifies from a single center, which appears during the 1st year of life and fuses to the remainder of the atlas by the 3rd year.31,34,53,86,87 A persistent bifid anterior and posterior arch of the atlas beyond age 4 years is observed in skeletal dysplasias, Goldenhar syndrome, Down syndrome, Conradi syndrome, and atlas assimilation.88 In an extensive review of CT scans from 1104 patients, Senoglu and colleagues89 found a 3.35% incidence. None had neurologic deficits or needed intervention. Rarely, hyperplasia of the posterior arch occurs and has been associated with myelopathy.90
There is varying loss of height of the atlas, allowing the odontoid to project upward into the foramen magnum and creating a “relative” basilar impression (see Fig. 30–14). The position of the odontoid relative to the foramen magnum was described earlier (see section on basilar impression). McRae38,83 measured the distance from the posterior aspect of the odontoid to either the posterior arch of the atlas or the posterior lip of the foramen magnum (SAC), which was closer. He stated that a neurologic deficit would be present if this distance was less than 19 mm. This distance should be determined in flexion because this position most dramatically reduces the space available for the cord.
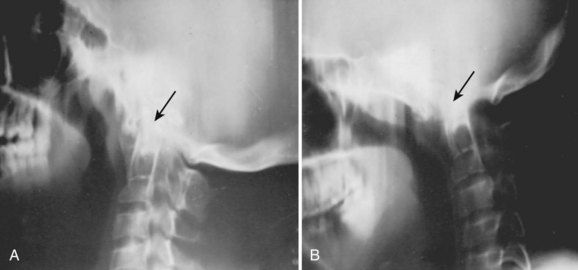
Flexion-extension stress films (see Fig. 30–14) often show posterior displacement of the odontoid from the anterior arch of the atlas of 12 mm.83 Associated atlantoaxial instability has been reported to develop eventually in 50% of patients29,31; this is determined by measuring the distance from the anterior border of the odontoid to the posterior aspect of the anterior arch of the atlas. A distance greater than 4 mm in young children who probably have considerable cartilage present and 3 mm in older children and adults is considered pathologic.86,87,91 The odontoid itself often has an abnormal shape and direction; it frequently is longer, and its angle with the body of the axis is directed more posteriorly.73,83
McRae33 was the first to note the frequent occurrence of congenital fusion of C2-3 (70%) and C1-2 instability in patients with atlanto-occipital fusion (Fig. 30–15). This occurrence suggests that greater demands are placed on the atlantoaxial articulation, particularly in flexion and extension when the joints above and below are fused.37,83 von Torklus and Gehle31 noted that approximately 50% of patients develop late onset of atlantoaxial instability and the resultant potential for compromise of the spinal cord.29

Gholve and colleagues32 used a morphologic classification: zone 1, a fused anterior arch; zone 2, fused lateral masses; zone 3, a fused posterior arch; and a combination of fused zones. In their study, 57% had atlantoaxial instability, with almost half of those having an associated C2-3 fusion. Spinal canal encroachment occurred in 37%, with almost half of these patients having clinical findings of myelopathy. The highest prevalence of spinal canal encroachment (63%) was noted in patients with occipitalization in zone 2.
Another commonly associated abnormality is the presence of a constricting band of dura posteriorly. This band has been found to create a groove in the spinal cord and may be the primary cause of symptoms. The band cannot be visualized on routine radiographs, and it does not correlate with the presence or absence of the posterior bony fringe of the atlas. Consequently, CT and MRI should be an integral part of the evaluation. Water-soluble contrast material (metrizamide) alone or in conjunction with CT can visualize the spinal canal and its contents. A properly performed study yields valuable information regarding the presence of a dural band; tonsillar herniation; and the size, shape, and position of the spinal cord in the spinal canal.35,92
Treatment
Management of this uncommon problem may be hazardous. In contrast to anomalies of the odontoid, surgical intervention carries a much higher risk of morbidity and mortality.37,73,93 Nonoperative methods such as cervical collars, braces, plaster, and traction should be attempted initially in some patients. These methods are often helpful in patients with persistent complaints of head and neck pain and are particularly helpful if symptoms follow minor trauma or infection. If neurologic deficits are present, immobilization may achieve only temporary relief. Patients presenting with evidence of a compromised situation in the upper cervical area must take precautions not to expose themselves to undue trauma.
With anterior spinal cord signs and symptoms owing to an unstable atlantoaxial complex, an occiput-to-C2 fusion is suggested, with preliminary traction to attempt reduction, if necessary. If reduction is possible and there are no neurologic signs, surgical intervention carries an improved prognosis.34,37,73 Operative reduction should be avoided because this has frequently resulted in death.72,73
Transoral resection of the odontoid should be considered if there is irreducible ventral compression.28,94 Resection of the odontoid through an anterior approach may destabilize the upper cervical spine. In a large study, Dickman and colleagues95 noted that 11 of 19 patients (40%) developed craniovertebral junction instability after transoral removal of the odontoid, 8 of whom did not have clinical or radiographic evidence of instability preoperatively. Instability was more common if there was a congenital bony malformation or if the patient required posterior decompression for an associated condition, such as Chiari malformation or syrinx.95
Posterior signs and symptoms and myelographic evidence of bony or dural compression, depending on the degree of neurologic involvement, may be indications for a posterior decompression and stabilization of the occiput to C2.71,96–99 Satisfactory occipital cervical stabilization and fusion can be obtained by using a halo brace in the postoperative period.98 Internal fixation can facilitate postoperative management for certain patients, however. Internal fixation of the occipital cervical junction can pose problems, and several fixation techniques have been found helpful.27,28,71 The addition of a cervical laminectomy may increase C1-2 instability or lead to the late development of a cervical kyphosis, particularly if the laminectomy involves several levels.96,100 In these cases, the patient should be managed expectantly with appropriate internal stabilization or a halo vest.82,96
Anomalies of Ring of C1
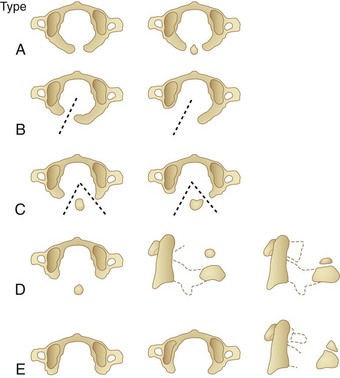
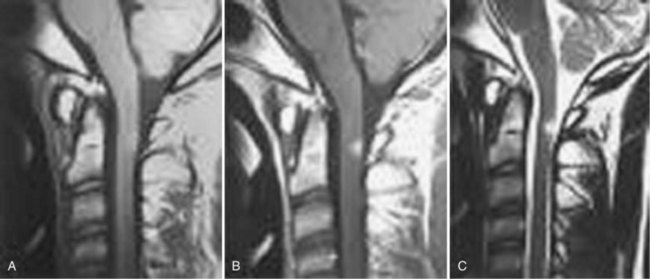
Anomalies of the posterior arch can be characterized as median clefts or hypoplasia. Geipel101 found defects in the posterior arch, most of which were median clefts, in 4% of 1613 autopsies. Currarino and colleagues102 developed a classification scheme (types A to E) for congenital defects of the posterior arch of C1 (Fig. 30–16). Greater than 90% are the type A median cleft variant. These patients are usually asymptomatic, and their anomaly is incidentally identified on radiographic studies.89 Types C and D are accompanied by a free-floating posterior tubercle. These patients may experience neck pain and neurologic symptoms before discovery of the anomaly. The free posterior tubercle has been shown to move with neck extension and in some cases may migrate anteriorly and traumatize the spinal cord with neck extension. MRI studies have shown signal abnormality of the posterior spinal cord at the C1-2 level consistent with this mechanism of injury (Fig. 30–17).102
Dubousset103 called attention to a previously unrecognized problem with the ring of C1, the hemiatlas. Although there had been an occasional case report, Dubousset103 presented the first large study to review the problem in depth. He reported 17 patients in whom he was able to document absence of the facet of C1, which led to a severe and progressive torticollis in young children (Fig. 30–18). Initially, the deformity is flexible and can be passively corrected. As the child ages, the torticollis becomes more severe and eventually fixed. Radiographic diagnosis using tomography or CT has been helpful in identifying this deformity. Use of traction to align the head and neck at the time of the study assists in highlighting the problem. If the patient is passively correctable, a single posterior fusion, occiput to C2, is performed. A halo cast is applied postoperatively to maintain the head in a satisfactory alignment until the fusion is complete.
Although the time at which this becomes a fixed deformity was not defined, Dubousset103 reported good results in teenagers. This deformity can accompany Klippel-Feil syndrome with anomalies of the lower cervical spine as well. Dubousset103 found an increased incidence of anomalies of the vertebral vessels in these children and suggested arteriographic evaluation before the use of traction or surgical intervention, which could further compromise a precarious blood supply to the midbrain and spinal cord.
Anomalies of Odontoid (Dens)
Congenital anomalies of the odontoid can lead to an unstable atlantoaxial complex, with potential neurologic sequelae and death owing to spinal cord pressure.50 Several gradations or variations of anomalies of the odontoid exist, ranging from aplasia (complete absence) to hypoplasia (partial absence) to os odontoideum (Fig. 30–19).
Aplasia or agenesis of the odontoid is a complete absence of development. Hypoplasia is a partially developed odontoid, ranging in size from a short, stubby, peglike projection to an odontoid of almost normal size.104 Os odontoideum is an anomaly in which the odontoid process is divided by a wide transverse gap, leaving the apical segment without support from the base.105 Distinguishing aplasia or hypoplasia from os odontoideum is of limited importance because these anomalies usually lead to atlantoaxial instability and the clinical signs, symptoms, and treatment are identical. The only distinctive features are radiographic.
Incidence
In the authors’ experience, aplasia is extremely rare. Many previous reports have confused aplasia for hypoplasia, and, as previously emphasized, aplasia probably has been a misnomer because it almost never describes an associated absence of the portion below the articular facets that contributes to the body of the axis. Hypoplasia and os odontoideum are infrequently reported and can be considered rare.54,104,106–109 With more recent awareness, these lesions are being recognized more commonly, however, than previous literature might indicate—especially os odontoideum.47 In a large series reported by Wollin,109 the average age of diagnosis was 30 years, but in a later series it was 18.9 years, suggesting earlier recognition.47 An increasing number of children with these anomalies are being discovered.
In conditions such as Down syndrome, Morquio syndrome, Klippel-Feil syndrome, and some skeletal dysplasias, odontoid anomalies in association with ligamentous laxity producing atlantoaxial instability are much more common than in the general population.40,42,50,110–115 Associated regional malformations may occur, but in contrast to many congenital cervical anomalies, they are rare.50,104,108,116
Development of Odontoid
The body of the odontoid is derived from the mesenchyme of the first cervical sclerotome and is actually the centrum of the first cervical vertebra, which becomes separated from the atlas during development to fuse with the remainder of the axis.82,114,117 The apex of the odontoid process is derived from the mesenchyme of the most caudal occipital sclerotome or proatlas. Ossification of these two segments of the odontoid proceeds along separate lines.
Between the 1st and 5th prenatal months, the dens begins to ossify from two centers, one on each side of the midline. By the time of birth, they have fused into a single mass.86,87,91 Occasionally, the right and left halves of the odontoid are not fused at birth, and a longitudinal midline cleft may be seen. At birth, the tip of the odontoid has not ossified, is V-shaped, and is known as a dens bicornis (Fig. 30–20). A separate ossification center within the “V,” known as a summit ossification center or ossiculum terminale, usually appears at age 3 years and fuses with the remainder of the dens by age 12.86,87,118 Cattell and Filtzer64 found an ossiculum terminale in 26% of 70 normal children 5 to 11 years old.
< div class='tao-gold-member'>

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


