Chapter 74 Compartment Syndromes and Volkmann Contracture
Anatomy
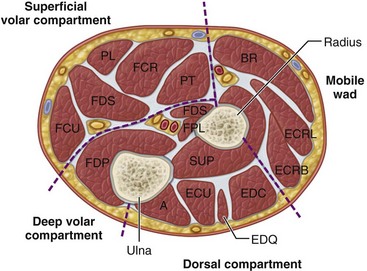
Four interconnected compartments of the forearm are recognized (Fig. 74-1): (1) the superficial volar compartment, (2) the deep volar compartment, (3) the dorsal compartment, (4) and the compartment containing the mobile wad of Henry (brachioradialis and extensor carpi radialis longus and brevis). The volar compartments are most commonly involved, but the dorsal and mobile wad compartments can be involved alone or in addition to the volar compartments. Clinically differentiating isolated or combined involvement of the deep and superficial volar compartments usually is difficult; however, the deep volar compartment (flexor digitorum profundus, flexor pollicis longus, and pronator quadratus) may be solely involved.
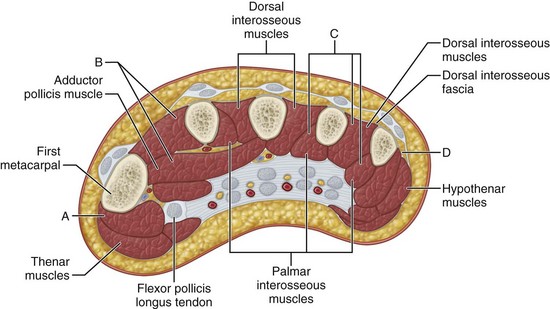
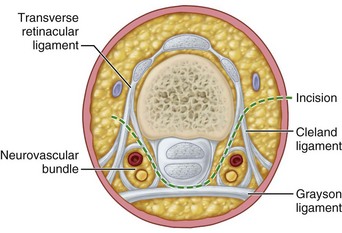
In the hand, each interosseous muscle is surrounded by a tough investing fascial layer, each making an individual compartment as shown by the injection dissections of Halpern and Mochizuki. The adductor pollicis muscle and the thenar and hypothenar muscles form three separate compartments (Fig. 74-2). The neurovascular bundles of each digit also are compartmentalized by fascial layers, making them vulnerable to excessive swelling (Fig. 74-3).
Etiology
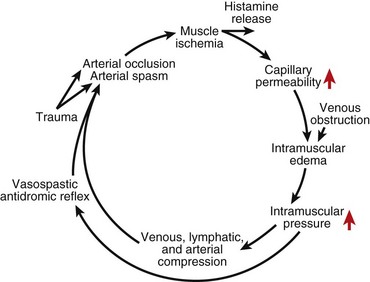
Any situation that causes a decrease in compartment size or increase in compartment pressure can initiate compartment syndrome. As the intracompartmental pressure increases, capillary blood perfusion is reduced to a level that cannot maintain tissue viability. The increase in interstitial pressure overcomes the intravascular pressure of the small vessels and capillaries, causing the walls to collapse and impeding local blood flow. In a canine model, muscle necrosis was shown to occur with a rise in pressure to within 20 mm below diastolic pressure. The local tissue ischemia leads to local edema, which increases intracompartmental pressure. This cycle of increasing muscle ischemia was depicted by Eaton and Green as shown in Figure 74-4.
Diagnosis
Measuring Compartment Pressures in the Forearm and Hand Using a Hand-Held Monitoring Device











Management
Acute Compartment Syndrome of the Forearm
Forearm Fasciotomy and Arterial Exploration
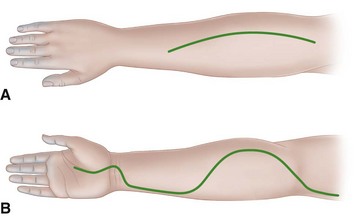
 For the volar fasciotomy, make a curvilinear incision similar to McConnell’s combined exposure of the median and ulnar nerve neurovascular bundles as described by Henry (Fig. 74-5). Make an anterior curvilinear incision medial to the biceps tendon, crossing the elbow flexion crease at an angle. Carry the incision distally into the palm to allow for a carpal tunnel release, but avoid crossing the wrist flexion crease at a right angle.
For the volar fasciotomy, make a curvilinear incision similar to McConnell’s combined exposure of the median and ulnar nerve neurovascular bundles as described by Henry (Fig. 74-5). Make an anterior curvilinear incision medial to the biceps tendon, crossing the elbow flexion crease at an angle. Carry the incision distally into the palm to allow for a carpal tunnel release, but avoid crossing the wrist flexion crease at a right angle.
 Divide the lacertus fibrosus proximally, and evacuate any hematoma.
Divide the lacertus fibrosus proximally, and evacuate any hematoma.







 Do not close the skin at this time; anticipate secondary closure later.
Do not close the skin at this time; anticipate secondary closure later.