CHAPTER 36 Cervical Spondylosis
Pathophysiology, Natural History, and Clinical Syndromes of Neck Pain, Radiculopathy, and Myelopathy
Degenerative changes at the cervical discs and facet joints are ubiquitous in the adult population; these changes are a natural consequence of aging and are asymptomatic in most of the population. Spondylosis refers to these age-related degenerative changes within the spinal column.1 Most patients who present with cervical spondylosis are older than 40 years.2 Although most of these age-related degenerative changes remain asymptomatic, they can manifest as three main symptom complexes—axial neck pain, upper extremity radiculopathy, or myelopathy—or some combination thereof.1
Pathoanatomy
Degenerative changes within the cervical disc lead to loss of disc height, arthrosis in the uncovertebral and facet joints, and motion aberrations between two vertebral bodies.3 In most patients, desiccation of the disc initiates a cascade of degenerative changes.4 An alteration in proteoglycan content beginning in the 3rd decade diminishes the ability of the disc to maintain its hydration.1 The amount of keratin sulfate increases, and the amount of chondroitin sulfate decreases.4 With these changes in viscoelasticity, the periphery of the disc begins to bear an increasingly greater proportion of the load borne by the disc, with resultant loss of disc height and bulging of the anulus into the spinal canal.
As the disc loses height, the vertebral bodies approach each other, causing infolding of the ligamentum flavum and facet joint capsule and reducing the dimensions of the canal and the foramen.5 The anterior height of the disc is greater than the posterior height of the disc in a normally configured disc; with degeneration, the ventral portion of the disc loses height to a greater degree than the dorsal portion, and loss of cervical lordosis can occur.6 A positive feedback cycle ensues with greater force placed on the ventral aspect of the vertebral bodies leading to kyphosis.4 The uncovertebral and facet joints bear greater loads, accelerating the formation of osteophytes at these joints and at the peripheral vertebral endplate margins. Osteophytes, the posteriorly protruded disc material, and the infolded soft tissue within the canal and neuroforamina all diminish the space available for the spinal cord or nerve root. Radiographically, the C5-6 interspace is the most frequently affected level, followed closely by C6-7.7
Pathophysiology
Pathophysiology of Axial Neck Pain
Axial neck pain results from a multitude of potential causes and can be divided geographically into anterior neck pain, which usually stems from sprains and strains of the sternocleidomastoid and other strap muscles and their attachments, and posterior neck pain, which can be subdivided further into subaxial and suboccipital locations.8 In many patients, subaxial neck pain results from muscular or ligamentous imbalances related to poor posture, faulty ergonomics, or muscle fatigue or stress or both. Muscular pain often occurs as a result of postural adaptations to a primary pain source located in the shoulder, the craniovertebral junction, or the temporomandibular joint.5
The physiology of this pain process is not yet fully delineated. Patients with chronic myofascial pain have significantly lower levels of high-energy phosphates in the involved muscle tissue.9 It is unknown whether the diminished level of high-energy phosphates causes the pain or if it is a result of the pain. Unencapsulated free nerve endings in the neck musculature function as chemonociceptive units. Fatigued muscle generates anaerobic metabolites, which accumulate and can stimulate these chemonociceptive nerve endings. These free nerve endings also respond to non-neurogenic pain mediators released as a result of ischemia or injury, such as bradykinin, histamine, serotonin, and potassium ions. Primary muscle pain may result from sensitization of these nerve endings.
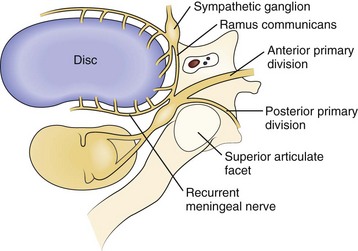
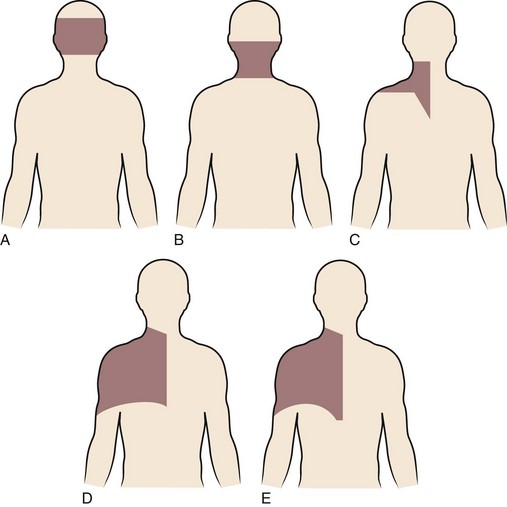
Axial neck pain should be attributed to degenerative changes in the cervical discs or facet joints only after careful consideration, owing to the ubiquitous nature of these changes in the spine. Nevertheless, multiple studies suggest that cervical discs and facet joints can generate pain.10–14 Nerve fibers and nerve endings, containing somatic afferent fibers, innervate the peripheral portion of the intervertebral disc (the outer third of the anulus) and offer a potential mechanism by which degenerative cervical discs generate pain directly. The sinuvertebral nerve, formed by branches of the ventral nerve root and by the sympathetic plexus, innervates the intervertebral disc (Fig. 36–1). When formed, the sinuvertebral nerve turns back into the intervertebral foramen along the posterior aspect of the disc, supplying portions of the anulus, posterior longitudinal ligament, periosteum of the vertebral body and pedicle, adjacent epidural veins, and dura mater.10 A review of a 12-year cervical discography experience suggests that stimulation of each disc results in consistent and predictable patterns of neck pain (Fig. 36–2).14
Degenerative changes at a cervical facet joint can be a source of axial neck pain. Provocative injections into the facet joints of asymptomatic volunteers result in a reproducible pattern of axial neck pain and shoulder girdle pain (Fig. 36–3).12 Controlled injection of anesthetic into the symptomatic facet joint or into the dorsal primary rami blocks these patterns of facet pain, suggesting that the facet joint plays a role in the development of axial neck pain. C3-4 to C8-T1 facet joints receive their innervation from the medial branches of the cervical dorsal rami above and below each joint, whereas the third occipital nerve innervates the C2-3 facet joint.11 The presence of mechanoreceptors and nociceptive nerve endings in cervical facet joint capsules further supports a possible role for these structures in the pathogenesis of cervical spine pain.15 Immunohistochemical studies show the presence of free nerve endings reactive for pain-related peptides located in the synovial folds of the human cervical facet joint.
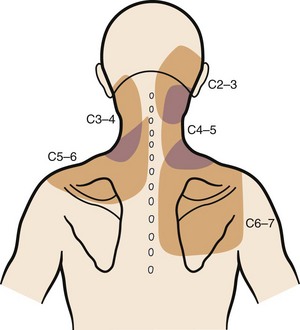
FIGURE 36–3 Composite map of axial pain patterns from facet joints at C2-3 to C6-7.
(From Dwyer A, Aprill C, Bogduk N: Cervical zygapophyseal joint pain patterns. I. A study in normal volunteers. Spine [Phila Pa 1976] 15:453-457, 1990.)
Suboccipital pain radiating down into the neck or to the back of the ear may be a manifestation of degenerative arthritis in the upper cervical spine. Injection of the atlanto-occipital and atlantoaxial joints results in a reproducible pain pattern in this region, with the atlanto-occipital joints showing the capacity to generate intense and diffuse pain.16 Wächli and colleagues17 reported unilateral headaches and atypical facial pain as a result of degenerative changes at the C2-3 level. Some patients with suboccipital headaches presumably have irritation of the greater occipital nerve, which originates from the posterior rami of C2, C3, and C4.18 The sinuvertebral nerves from C2 and C3 exist as another potential source of suboccipital pain, ascending proximally to innervate the atlantoaxial ligaments, tectorial membrane, and dura mater of the upper cervical cord and posterior cranial fossa.10
Pathophysiology of Radiculopathy
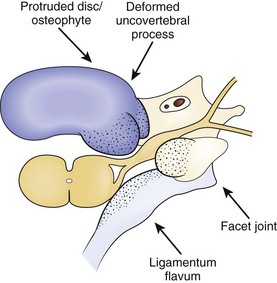
Radicular findings in the arm originate from the cervical nerve roots at some point between their origins as nerve rootlets from the spinal cord and their transition into peripheral nerves as they emerge from the neural foramen. Degenerative changes at the cervical motion segment, soft disc herniations, stenosis, intrinsic nerve root pathology, and trauma all can result in these symptoms. Loss of disc height leads to impingement on the nerve root origins from disc bulging, infolding of the facet joint capsule and ligamentum flavum, and osteophyte formation at the disc margins (hard disc formation) and at the uncovertebral and facet joints, all of which result in foraminal stenosis and radiculopathy (Fig. 36–4). Osteophytic spur formation may also compromise the blood supply to the nerve roots. Osteophytes may compress radicular arteries within the dural root sleeves leading to spasm and reduced vascular perfusion. Additionally, blockage of venous outflow may occur, resulting in edema and further compromise of the blood supply of the nerve roots.19
Mechanical deformation of the nerve root may lead to motor weakness or sensory deficits. The exact pathogenesis of radicular pain is unclear, but the general belief exists that in addition to the compression, an inflammatory response must occur for pain to develop. Within the compressed nerve root, intrinsic vessels show increased permeability, secondarily resulting in edema of the nerve root. Chronic edema and fibrosis (scar) within the nerve root play a role in altering the response threshold and heighten the sensitivity of the nerve root to pain.20 Neurogenic chemical pain mediators released from the sensory neuron cell bodies and non-neurogenic mediators released from disc tissue may initiate and perpetuate this inflammatory response (Table 36–1).21,22
TABLE 36–1 Chemical Mediators of Spinal Pain
| Neurogenic | Non-neurogenic |
|---|---|
| Substance P | Bradykinin |
| Somatostatin | Serotonin |
| Cholecystokininlike substance | Histamine |
| Vasoactive intestinal peptide | Acetylcholine |
| Calcitonin gene-related peptide | Prostaglandin E1 |
| Gastrin-releasing peptide | Prostaglandin E2 |
| Dynorphin | Leukotrienes |
| Enkephalin | diHETE |
| Gelanin | |
| Neurotensin | |
| Angiotensin II |
diHETE, dihydroxyeicosatetraenoic acid
From Chabot MC, Montgomery DM: The pathophysiology of axial and radicular neck pain. Semin Spine Surg 7:2-8, 1995.
Dynamic factors in the cervical spinal column affect the amount of nerve root compression. Flexion of the cervical spine lengthens the cervical neural foramina 18% to 31%, whereas extension shortens the foramina 16% to 22%.23 Rotation to the ipsilateral side narrows the foramen, whereas rotation to the contralateral side widens the foramen. The facet joint capsule and ligamentum flavum buckle with extension, narrowing the foraminal dimensions further. Translation or angulation between vertebral bodies in flexion or extension may result in increased stretch on the nerve root and predispose the individual to radicular symptoms. Patients who do not have nerve root compression with their necks in a static, neutral position may dynamically compress the nerve root during normal activities, resulting in radicular symptoms.
Changes in intrinsic tension within the nerve root have the ability to alter radicular pain. Davidson and colleagues24 postulated that the decrease in tension within the nerve root caused by a patient resting the hand atop the head—the shoulder abduction sign—relieves radicular pain. These investigators also postulated that this change in arm position lifts the sensory root, or dorsal root ganglion, directly cephalad or lateral to the source of compression and that this position decompresses the epidural veins, augmenting pain relief. Another study suggested that the abducted arm position allows relative laxity in the dural ligaments (of Hoffman), resulting in decreased tension on the nerve root.25
Often, patients present with radicular pain in an atypical distribution.26 An anatomic human cadaveric study confirmed the high incidence of intradural connections among C5, C6, and C7 dorsal rootlets (noted to be anatomic variants because of their high incidence rather than anatomic anomalies) and postulated that these variant intradural connections potentially explain the clinical variation and overlapping sensory symptoms frequently observed with cervical spine nerve root compression.27
Pathophysiology of Myelopathy
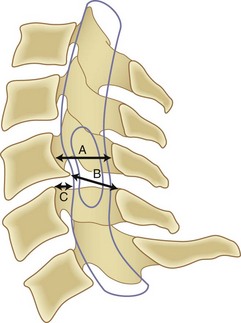
Although it is generally agreed that mechanical compression of the spinal cord is the primary pathophysiologic mechanism resulting in myelopathy, in many patients a combination of this static compression with dynamic factors secondary to motion between the vertebral bodies, a congenitally stenotic canal, changes in the intrinsic morphology of the spinal cord, and vascular factors contributes to the development of myelopathy. A developmentally narrow spinal canal in the anteroposterior plane can contribute to the development of cervical myelopathy. The normal anteroposterior diameter of the cervical spine measures 17 to 18 mm in adults, and the anteroposterior diameter of the spinal cord in the cervical region measures approximately 10 mm. An anteroposterior diameter of the spinal canal less than 13 mm defines congenital cervical stenosis, whereas a diameter greater than 16 mm suggests a relatively low risk of myelopathy (Fig. 36–5A).28,29 A congenitally narrow spinal canal lowers the threshold at which the cumulative effects of various degenerative structures encroaching on the spinal cord cause signs and symptoms of myelopathy.30
A strong association exists between flattening of the cord within the narrowed spinal canal and the development of cervical myelopathy. Penning and colleagues31 believed that symptoms of cord compression occurred when cross-sectional area of the cord had been reduced by a critical amount (30%) and the remaining transverse area of the cord was less than 60 mm2. Houser and colleagues32 contended that the extent and shape of flattening of the spinal cord serve as an indicator of neurologic deficit: 98% of their patients with severe stenosis manifested by a banana-shaped spinal cord had clinical evidence of myelopathy. Ono and colleagues33 described an anteroposterior cord compression ratio calculated by dividing the anteroposterior diameter of the cord by the transverse diameter of the cord. A lower anteroposterior compression ratio (<0.40) correlated well with the areas of most severe injury of the cord histologically. The Pavlov ratio, which is the anteroposterior diameter of the spinal canal divided by the anteroposterior diameter of the vertebral body at the same level, as measured on a lateral radiograph, also indicates static compression; a value of 0.8 or less indicates a developmentally narrow cervical canal and stenosis of the canal.30,34
Segmental motion of the cervical spinal column affects the development of cervical myelopathy. Hyperextension of the neck narrows the spinal canal by shingling the laminae and buckling the ligamentum flavum ventrally into the canal. Extension and flexion of the neck may alter the diameter of the canal by 2 mm.35 Angulation or translation between vertebral bodies in flexion or extension may result in narrowing of the space available for the cord (Fig. 36–5B). Particularly during extension, retrolisthesis of a vertebral body can pinch the spinal cord between the inferoposterior margin of a vertebral body and the superior edge of the lamina caudad to it. Forward slippage of a vertebral body may compress the spinal cord between the superoposterior margin of the vertebral body below and the lamina above.30 Flexion of the spinal column aggravates this forward slippage. Retrolisthesis and anterolisthesis often cause myelopathy in elderly (≥70 years old) patients (Fig. 36–5C).28,36 Additionally, hypermobility at the third and fourth cervical levels cephalad to a degenerated and stiffened C4-5 segment commonly exists in elderly individuals, potentially resulting in myelopathy at the hypermobile C3-4 level.37 Research using a spinal cord model showed that the cord is more vulnerable to dynamic, repeated minor loading compared with severe static loading.38
Cervical spine flexion and extension cause morphologic changes within the spinal cord itself. Breig and colleagues39 showed that the spinal cord thickens and shortens with extension, which renders it more susceptible to pressure from the infolded ligamentum flavum or lamina. The spinal cord stretches with flexion, which may subject the cord to higher intrinsic pressure if it presses against a disc or a vertebral body anteriorly. Flexion of the cervical spine may cause stretch (strain) injury to the axons through tensile loading, resulting in increased permeability and myelin injury, rendering these already injured axons more susceptible to secondary injury from other processes, including ischemia.40
Barre41 first proposed in 1924 the possibility that vascular factors play a significant role in the development of cervical myelopathy. The acute development or progression of findings suggests vascular involvement. In two separate canine experiments, cervical cord ischemia superimposed on compression of the cord resulted in a dramatic increase in neurologic findings.42,43 The effects of compression and ischemia were additive and responsible for the clinical manifestations of myelopathy. These investigations also led to the proposal that ischemia may play an important role in the irreversibility of spinal compression.42 In a separate dog study, obstruction of the peripheral arterial plexus caused structural changes within the spinal cord.44
The classic study by Breig and colleagues39 established that blood flow through the anterior spinal artery and anterior radicular arteries diminishes when those vessels are tented over a disc or a vertebral body, but that this position does not have a substantial impact on flow through the tortuous posterior spinal arteries. Vessels considered most vulnerable to reduced blood flow include the transverse intramedullary arterioles, arising from the anterior sulcal arteries. These vessels perfuse the gray matter and adjacent lateral columns.45 Ischemia may also occur from venous congestion.46 One cell type known to be particularly sensitive to ischemic injury, the oligodendrocyte, plays a principal role in insulating axons with a myelin sheath. Oligodendrocyte death caused by ischemic insult, likely through the mechanism of oligodendrocyte apoptosis, may explain the demyelination and subsequent irreversible neurologic deficit associated with chronic cervical myelopathy.40,47
Severe compression results in pathologic changes within the spinal cord. The central gray matter and the lateral columns show the most changes, with cystic cavitation, gliosis, and demyelination most pronounced caudad to the compression site. The posterior columns and posterolateral tracts show wallerian degeneration cephalad to the site of compression. The irreversibility of these changes may explain why some patients fail to recover after decompressive surgery. The anterior white columns are relatively resistant to infarction, even in cases of severe compression.48
Natural History and Epidemiology of Neck Pain, Radiculopathy, and Myelopathy
Axial Neck Pain
Neck pain commonly affects adults of all ages and both sexes almost equally. Few population-based studies exist on the prevalence of neck pain. A study of the Saskatchewan adult population showed that neck pain is more prevalent than commonly thought, with 66% of adults experiencing neck pain during their lifetime and 5% highly disabled by it.49 Another study showed a 9% point prevalence of neck and shoulder pain.50 The prevalence of neck pain increases in highly educated individuals and in individuals with a history of injury, headaches, low back pain, or medical comorbidities such as cardiovascular and digestive disorders.51
No true natural history studies of axial neck pain exist; all published studies involve some form of treatment in most patients. DePalma and Subin52 found that most patients with axial symptoms from cervical spondylosis respond favorably to nonoperative treatment. After 3 months of nonoperative treatment, 29% of their patients had total relief of symptoms, 49% improved, and 22% did not improve. Rothman and Rashbaum53 reported on the 5-year outcome of patients with “predominantly” axial neck pain treated conservatively. They found that 23% of these patients remained partially or totally disabled from their symptoms. At the 5-year follow-up, Rothman and Rashbaum53 found no significant difference between this group and another similar group of patients who underwent surgery and recommended nonoperative management for “non-neurogenic” axial neck pain symptoms.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


