Chapter 42 Canes, crutches, and walkers
Assistive devices for ambulation have historical precedents, having been used since the Neolithic period. Whether necessitated by injury or disease or by the need to traverse rocky, hilly terrain, early people devised supports to enable them to get about, to sidestep starvation, and to evade predators. An ancient Egypt carving on the entrance portal of Hirkouf’s tomb dating to the Sixth Dynasty (2830 BCE) depicts a figure leaning on a crutch-like staff (Fig. 42-1).38,70 The contemporary bishop’s staff, royal scepter, academic mace, and the walking stick used to climb The Great Wall in China are modern versions of the basic support. The crutch remained a simple T design until approximately 1800, when use of the saw enabled modifications, such as splitting the staff, spreading the two halves, and inserting a cross-piece for the hand. The cane or walking stick was essential to the wardrobe of the stylish eighteenth- and nineteenth-century physician.44

New materials and designs, greater knowledge of biomechanics and pathology, and changing demographics and social mores have led to a myriad of cane, crutch, and walker designs. The expansion of the geriatric segment of the population gives assistive devices greater visibility. For all ages, the mandate of the Americans with Disabilities Act has prompted developers to use ingenuity to create appliances fostering easier access by people with disabilities. No longer is it a rarity to see someone in a shopping mall using a walker. Mobility-related assistive technology can be obtained through Medicare’s durable medical equipment benefit.136 Nevertheless, a national sample of 3,485 older Americans showed that income and insurance affect the use of canes and other assistive devices.78 Assistive technology can enable many people to continue or resume ambulatory function at the maximum level possible.59
Assistive devices serve one or more functions:
Canes
Unlike the walking stick, which usually is a straight shaft, perhaps topped by an ornamental knob, the cane used in rehabilitation has a handle. A broad array of manufactured handles is available. The basic crook handle enables the person to hang the cane over the forearm or the back of a chair. One ergonomically shaped handle (available at www.CanesCanada.com) is designed to contact more of the hand, thus contributing to the user’s comfort. The handle is made for right and left hand use. The Right-Grip (available at www.fetterman-crutches.com) has a contoured handle designed to keep the wrist in neutral posture rather than in dorsiflexion.
Cane shafts may be solid, height adjustable, or folding. The folding shaft makes storage more convenient; an adult-size cane can be folded to approximately 30.5 cm (1 foot). The SuperCane (Momentum Medical Corp., Idaho Falls, ID) has an offset shaft with a higher hand grip to be used when the patient walks and a lower hand grip that enables the person to start the standing maneuver while seated. A novel cane has a shaft containing a weight-measuring system and a feedback mechanism in the handle; the cane informs the user by vibration or lights as to the amount of weight borne, useful for those who need to limit loading on an affected leg.37
The base of the cane usually is the distal end of the shaft and terminates in a rubber tip. A spring-loaded tip absorbs shock at initial contact. The AbleTripod (available at www.abletripodcane.com) has a flexible triangular tip that maintains floor contact at a wide range of shaft angles; the tip also absorbs shock. Retractable metal tips or spikes increase stability when the user walks on ice or snow.
Other base designs include the standard or wide-based quadruped (quad), which features a distal rectangle supporting four tips intended to increase the base of support.59 Patients with hemiplegia may not find the four-footed cane any more advantageous than a standard cane with a single tip.84 The Pilot rolling cane (available at www.FullLifeProducts.com) has an L-shaped base fitted with three casters that provide the user with the support of a quad cane without the need to lift the cane with each step. The cane also has a brake control in the handle for maximum stability. The Pilot step-up cane has a broad base with a flip-up platform that allows patients to maneuver over curbs and stairs without losing cane support. The user pushes a button on the handle to flip open the hinged platform; this enable the patient to step half the distance of the conventional 8-inch step. With the step retracted, the cane functions as a standard quad cane. The cane also has a second handle part way down the shaft that facilitates rising from toilets and other seats. The side walker/cane (available at www.tfihealthcare.com) has four widely spaced rubber tips that increase stability, especially when used unilaterally by a patient with hemiplegia.
The marketplace also has several novel cane-like designs intended for adults with lower-limb amputation. They enable the user to ambulate without a prosthesis. The Ed Walker (available at www.theedwalker.com) has a bicycle seat mounted on top of a vertical shaft. Jutting laterally is a second curved shaft, which has a platform for the amputation limb and terminates in a cane handle.28 The iWalkFree (available at www.fetterman-crutches.com) has a platform on a vertical shaft that supports the transtibial amputation limb or an injured lower leg. The wearer supports weight through the thigh and knee. Both devices have a stationary base. The Roll-A-Bout (available at www.roll-a-bout.com) terminates in four 8-inch wheels. This folding device has a cushioned platform for the lower leg and a handle that the user holds while propelling with the opposite foot.
A major class of canes is long canes with the lower portion of the shaft colored red. These canes are used by people with visual impairment.58,85,99,109 The shaft transmits to the user vibratory impulses regarding the terrain, while the red tip signals passersby not to impede the user.
Crutches
Crutches are of four major types (Figs. 42-2 and 42-3)59:
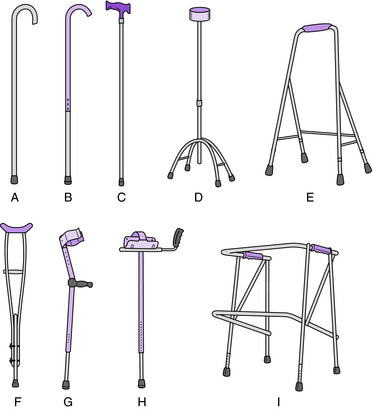
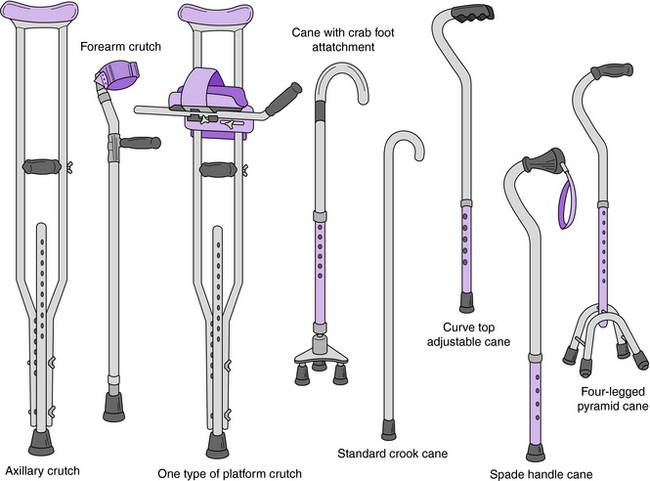
Underarm crutches, sometimes called axillary crutches, are made of wood, aluminum, and titanium in sizes made to fit children and adults. Metal crutches have spring-loaded detents that facilitate adjustment of hand grip height and overall length. The top of the crutch is erroneously termed the axillary piece. The axilla should never be used as a support area because superficial nerves and blood vessels may be compressed by direct pressure from the axillary piece. The top is often covered with sponge rubber to increase friction and cushion stress against the user’s chest. One design has a top resembling a shepherd’s crook more than twice the length of the basic top; this design offers more support area on the chest. The Easy Strutter Functional Orthosis (available at www.icanwalk.com) has a crutch top that includes, in addition to the underarm piece, a cushioned strap over the shoulder to distribute weight over a broad, pressure tolerant area. The crutch has two parallel struts that terminate in a broad, spring-loaded shock-absorbing base. When three-point gait with axillary crutches was compared with performance with the Easy Strutter Functional Orthosis, the latter crutches imposed less stress on the palms. Subjects reported feeling more secure on level surfaces and stairs with the new crutches.93
The crutch handle should have a resilient cover to cushion compressive stress on the palm. Whether the handle is cylindrical or wide, the palmar load distribution is similar.107
Although the traditional shaft bifurcates partway up from the base, streamlined single shaft canes are widely available. The usual crutch tip is rubber; however, many cane tips can be used on crutches. The Safe Walk (available at www.sailmarket.com/ticrutch) has two distal shafts both ending with rubber tips; one tip is always on the ground regardless of angle of the crutch. A spring-loaded mechanism at the distal end of the shaft absorbs considerable impact shock.96
Forearm (Lofstrand) crutches are made of aluminum or titanium with a vinyl-covered steel forearm cuff. They have adjustable length and cuff positions. European model cuffs are streamlined. They are sold in a wide variety of colors and can be ordered in a collapsible model for convenient storage. One innovation is a forearm crutch made of compliant composite plastic with an S curve in the shaft; the crutch design and material contribute to shock absorption.112
Crutches, regardless of design, are ordinarily used in pairs.
Walkers
Walkers are frames that provide bilateral support without the need to control two canes or crutches.
A variety of walkers are manufactured and are described based on their design59:
Many walkers with two front wheels and two crutch tips are available. The Red Dot walker (available at www.sunrisemedical.com) is a folding walker with two front-swivel 5-inch wheels and rear glide brakes. The Strider group of walkers (available at www.sammonspreston.com) has adjustable wheels and handles. Two-wheeled walkers may have tennis balls or other glides on the rear uprights to smooth ambulation. The WalkAbout has an upper portion that encircles the user.135 It also has a built-in seat and a basket. Other walkers with seats include the folding steel Merry Walker (available at www.merrywalker.com), Dura Walker (available at www.duralife-usa.com) made of polyvinylchloride, and the folding steel U-Step (available at www.ustep.com), which has a padded seat, hand brakes, and an optional laser light intended to encourage patients with Parkinson disease to step forward. A walker can have a reciprocating mechanism to accommodate stepping more easily. The Universal Stair Climbing Walker (available at www.tfihealthcare.com) facilitates ascending and descending steps.
Three-wheeled walkers have three angled uprights each ending in a wheel—an example is the Rollator (available at www.sammonspreston.com)—are easier to maneuver in narrow corridors. Basic wheeled and four-tip walkers are manufactured in wide size to suit obese patients.
Reverse walkers for children with cerebral palsy may facilitate hip and knee extension, allowing them to walk with less energy and a better faster gait. Some walkers for young patients allow hands-free ambulation. These appliances may provide mobility for children who are unable to support the trunk over the pelvis. Examples are the Mulholland Walkabout Gait Trainer (available at www.mulholland.com), Pony walker (available at www.gtkrehab.com.au), Rifton gait trainer (available at www.Rifton.com), and SMART Walker (available at www.llop.com). The SMART walker consists of a trunk–hip–knee–ankle orthosis worn with high-quarter, extra-depth laced-to-toe shoes. The orthosis is attached to a square-wheeled frame that has a steering mechanism designed to reduce neuropathic forces that cause scissoring and internal rotation.
Still under development is a robotic walker, the Veterans Affairs Personal Adaptive Mobility Aid (VA-PAMAID).101 Laboratory testing of the motorized device confirms durability and ease of use by elderly adults and those with visual impairment.
Measuring assistive devices
Whatever the device, the clinician must ensure that it fits properly.103,106,125 Correct height of the device and proper positioning of the handle or cuff enable the user to walk with the least effort and the greatest comfort.
Canes
Ordinarily, the single cane is held in the hand opposite the involved lower limb. First, remove the rubber tip by twisting on the shaft, not the handle. The patient stands with the elbow slightly flexed, no more than 30 degrees. Place the cane so that the end is 5 to 10 cm lateral and 15 cm anterior to the foot. The top of the handle should be at the wrist crease31,65,73,86 or the greater trochanter.110 After adjusting cane height, replace the rubber tip.
Canes that are too long cause the user to lean forward. Too short a cane imposes undue stress on the lumbosacral region. Shorter canes, however, enabled healthy subjects to perceive ground touch more accurately than with longer canes, suggesting that individuals with visual impairment will walk more safely with a slight decrease in cane length.114
Underarm crutches
Measure underarm crutches with the patient standing in a secure environment, such as between parallel bars. Each crutch should extend from a point approximately 4 to 5 cm (two finger breadths) below the axilla to a point on the floor 5 cm lateral and 15 cm anterior to the distal foot.95 Hand piece placement should enable the patient to have a 30-degree resting elbow flexion angle.100 Less flexion is suitable for the individual who walks by alternating foot steps.
In an alternative method used to determine crutch height, subtract 40 cm from the patient’s height16 or make the crutch equal to 77% of the subject’s height.14 When the person is supine, the crutch extends from 5 cm below the axilla to 5 to 7.5 cm from the lateral border of the heel.110 In the sitting position, the patient can abduct both arms to shoulder level and extend the elbows. Crutch length is the distance from the tip of the middle finger to the tip of the olecranon process of the opposite arm.88 An adjustable measuring crutch also can be used.119
Forearm crutches
The patient should stand with the crutch hand piece adjusted to provide 15 to 30 degrees of elbow flexion; more acute elbow flexion is required for gait patterns that require the user to lift both feet from the floor simultaneously. The crutch should contact the floor 5 to 10 cm lateral and 15 cm anterior to the toes. The cuff should lie on the proximal third of the forearm, approximately 2.5 to 4 cm below the olecranon process.110 A double-blinded repeated measures study of healthy subjects demonstrated that crutch length within 2.5 cm of the recommended length did not affect respiratory exchange ratio, walking speed, or perceived exertion.87
Triceps crutches
The upper cuff should contact the proximal third of the arm, approximately 5 cm below the anterior fold of the axilla. The lower cuff should lie 1 to 4 cm below the olecranon process to avoid bony contact yet provide adequate stability to the arm.110
Platform crutches
If the crutch has a forearm platform, it should be angled so that the user has maximum comfort and control of the crutch; ordinarily the forearm rests on the platform at a 90-degree angle to the upper arm. Measuring may be facilitated with use of special devices4 or variations on the techniques described.
Crutches that are too short compel the user to lean forward, whereas crutches that are too long force the shoulders up and risk compression of the radial nerve22,98,105 or suprascapular nerve.111 Even properly adjusted crutches, when used incorrectly, cause some patients to experience redness, pain, and abrasion of the lateral chest; tenderness over the medial aspect of the arm; cramping of the triceps; bruising of the medial epicondyle; shoulder pain; and ulnar neuropathy.
Gait patterns
Foot sequence determines the way an individual uses assistive devices.19,72,110 Selection of gait pattern(s) depends on the patient’s ability to move the feet reciprocally, tolerate full load on each leg, lift the body off the floor by pressing on the hands, and maintain balance. A gait pattern may be altered if the environment is crowded or the floor is slippery or sloping.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


