CHAPTER 30 Calcific Tendinitis
Calcific tendinitis of the shoulder is a self-limiting calcification of the rotator cuff. It can be categorized as an enthesopathy of the shoulder, and is characterized by inflammation around calcium hydroxyapatite crystal deposits, usually located in the supraspinatus tendon, near its insertion site. These radiologically evident calcific deposits have been reported in 2.7% to 20% of asymptomatic adult patients1,2 and in 6.8% of adult patients with shoulder pain.2 The discomfort associated with the calcification is believed to be caused by inflammation around calcium deposits located in or around the rotator cuff tendons. The process consists of a multifocal cell-mediated calcification of a living tendon that is usually followed by spontaneous phagocytic resorption.3 After resorption or surgical removal of the deposit(s), the tendon reconstitutes itself.4 When this condition becomes painful, it usually has an abrupt onset and can severely limit physical activity, even though its formation is not necessarily activity-dependent. It is believed that the disease only becomes acutely painful when the calcium is undergoing resorption.
The disorder is most common among people between 30 and 60 years old. Women are slightly more likely to be affected than men, and workers in sedentary jobs appear to be at higher risk than those in manual labor.5 Bilateral involvement is not uncommon. The diagnosis is made by history and physical examination, with specific attention to radiographic evidence of calcification. Patients usually exhibit specific tenderness over the greater tuberosity and symptoms similar to those of impingement syndrome.
HISTORICAL REVIEW
In 1907, Painter was the first to describe the radiographic findings in patients with calcific tendinitis of the shoulder.6 Codman discussed the problem in the 1930s and described the pathology as located primarily within the supraspinatus tendon, adjacent to the insertion on the greater tuberosity, but could also be found within the subscapularis, infraspinatus, and teres minor.7 In the 1940s, Bosworth reviewed radiographs and examined 6061 employees of an insurance company and found an incidence of 2.7% of calcific deposits in the shoulder. Of these, 51.5% of the deposits were in the supraspinatus tendon.8
PATHOGENESIS
Considerable controversy remains regarding the cause of this condition. Codman proposed that degenerative changes were necessary before the tendon would calcify.7 Conversely, Uhthoff and others do not believe that degeneration plays a role in calcium deposition, but that calcification is actively mediated by cells in a specific local environment; the age distribution and self-limiting course of the disease mitigates against degeneration as the cause.4
The disorder has four stages. The first, the precalcific stage, involves asymptomatic fibrocartilaginous transformation within the tendon. In the second stage, the formative stage, calcification develops within the cuff. This process may produce no symptoms or may be associated with variable degrees of pain at rest or on movement, especially abduction. The third stage, the resorptive stage, is the most incapacitating for patients, because extravasation of the calcium crystals into the subacromial bursa may cause constant severe pain and restriction of movement that typically lasts for 1 to 2 weeks. During this stage, systemic symptoms such as fever and malaise may be present. Some patients may even have elevated erythrocyte sedimentation rates and neutrophilia.9 The differential diagnosis in such patients includes joint sepsis and gout. The final stage, the postcalcific stage, involves healing and repair of the rotator cuff. This phase may last several months and may be associated with some pain and restriction of function.
Pain is thought to be an inflammation-induced response to the local chemical pathologic disorder and to direct mechanical irritation. Neer has described four possible causes for pain associated with calcium deposits.10 First is pain caused by chemical irritation induced by the calcium crystals. Most commonly, this presents as a bursitis, but may occasionally present as an inflammatory synovitis that can be clinically difficult to distinguish from septic arthritis. The second source of pain is pressure within the tissue as it swells, described by Codman as a “chemical furuncle.”7 The third is an impingement-type pain caused by bursal thickening and irritation. The fourth cause is the chronic stiffening of the joint (frozen shoulder), which may occur as a result of holding the affected arm continually at the side to avoid irritating the calcium deposit(s).
The most common site for occurrence is within the supraspinatus tendon and at a location 1.5 to 2.0 cm medial to the insertion on the greater tuberosity.4,10 Other affected sites include the infraspinatus, teres minor, and subscapularis tendon, in descending order of frequency. It almost always has an onset in those who are older than 30 years, and it affects up to 20% of the population. Up to 10% have bilateral involvement.11 Most patients are asymptomatic. Patients with diabetes are more likely to develop asymptomatic deposits; more than 30% of patients with insulin-dependent diabetes have tendon calcification.11 According to an arthrographic study,12 a rotator cuff tear may coexist in approximately 25% of patients presenting with calcific shoulder tendinitis. Surprisingly, small rather than large calcification deposits are more likely to be associated with cuff pathology.12
PRESENTATION
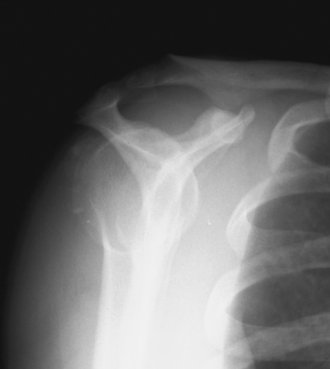
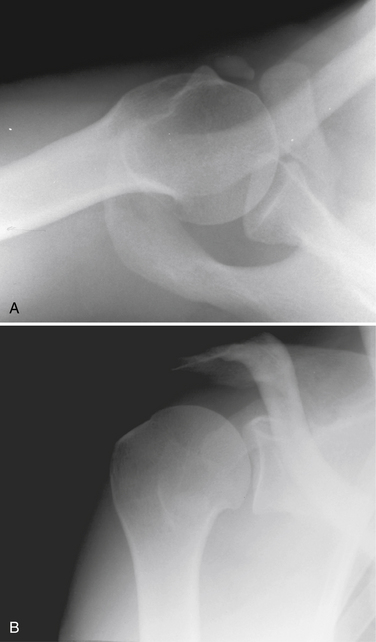
The diagnosis of calcific tendinitis is confirmed by radiographic evidence of calcification that is restricted to the tendon and usually does not affect he bone. Plain radiographs are valuable for two reasons. The first is for diagnosis and localization of the calcific deposit. The second is to follow changes during treatment. A routine shoulder series (anteroposterior [AP] views in internal rotation [IR] and external rotation [ER], outlet, and axillary) is initially obtained. These can be supplemented with additional views if further localization of calcium is needed. Calcium deposits located in the supraspinatus tendon can be seen on a true AP view of the glenohumeral joint (Fig. 30-1). Internal and external rotation AP views are used to localize deposits further in the infraspinatus and supraspinatus, respectively. In addition, a supraspinatus outlet view helps localize supraspinatus deposits to the anterior subacromial region and deposits in the infraspinatus to the posterior region (Fig. 30-2). Acromial morphology and the presence of any subacromial osteophytes are also detected on an outlet view. The axillary view is useful for identifying deposits within the subscapularis tendon (Fig. 30-3). The Zanca view for the acromioclavicular joint (10-degree cephalic tilt) is part of a routine shoulder series and the calcific deposit is often seen clearly. DePalma and Kruper11 have described calcifications on radiographs as dense and well defined in the formative stage, but cloudlike or irregular in the resorptive phase. Calcific tendinitis must be distinguished from dystrophic calcification associated with rotator cuff disease that occurs closer to the tendon insertion. The latter carries a worse prognosis and is not associated with the eventual resorption of calcium and resolution of symptoms. Stippled calcification or calcification that extends into bone is associated with glenohumeral arthropathy; such degenerative radiologic signs are rare in individuals with calcific tendinopathy.4

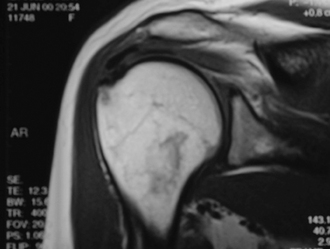
Magnetic resonance imaging (MRI) evaluation is not indicated routinely. The calcifications appear as areas of decreased signal intensity on T1-weighted images, whereas T2-weighted images may show an area of increased signal intensity surrounding the lesion similar to that of edema (Fig. 30-4).
TREATMENT OPTIONS
Although the disease has historically been considered to be self-limiting, spontaneous disappearance of periarticular calcifications was reported in only 9.3% of patients after 3 years and 27% after 10 years.13 Chronic pain is possible along with occasional acute flare-ups, which can cause significant morbidity. The treatment of calcific tendinitis is typically conservative, with the reported success rate between 30% and 85%.14
Nonoperative Treatment
Numerous nonsurgical approaches have been used to treat painful calcific tendinitis. The goal of therapy is to control pain and maintain function. During the acute and/or painful stage of the disorder, patients may need to rest the affected arm in a sling. During all phases of the disease, nonsteroidal anti-inflammatory drugs (NSAIDs) are a mainstay. Subacromial steroid injections may be beneficial if the patient shows impingement signs.15 Some authors recommend subacromial injections specifically during the formative (chronic) phase to relieve impingement pain.4 To the contrary, Lippmann has warned that corticosteroids may inhibit the cellular activity that produces disruption of the calcium deposit.16
Once pain is controlled, function may be maintained through exercises for range of motion and rotator cuff strengthening. There is mixed evidence that therapeutic ultrasound is more effective than placebo ultrasound for treating patients with calcific tendinitis.17

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


