ck=”if (window.scroll_to_id) { scroll_to_id(event,’R3-3′); return false; }” xpath=”/CT{06b9ee1beed5941901b763cd53362c21cc9ec01f975b9454417416ca7fe6c76fa3676cc20c20abb0ac0c9091fb223267}/ID(R3-3)” title=”3″ onmouseover=”window.status=this.title; return true;” onmouseout=”window.status=”; return true;”>3). It further seals the hip joint, creating a hydrostatic fluid pressure in the intra-articular space (4), and assists in dispersing the load if impingement between the femur and acetabulum occurs. Thickness of the joint capsule has also been linked to joint stability (5). The role of the joint capsule as a stabilizer is an especially important consideration in total hip arthroplasty (THA), as research has suggested that compromise of the capsule may be an important, if not the primary, cause of dislocation after arthroplasty surgery (1). As with all synovial joints, the structure of the hip joint is intimately related to its function. Although the basic architectural design of a given joint is the same among normal individuals, there are significant enough differences in the anatomical dimensions and shapes between individuals to allow for differences in precise function. Variations in anatomical characteristics of the hip joint have been observed to affect hip joint stability, mobility, and load at the joint. Consequently, anatomical features have implications for normal hip joint function during various activities as well as dysfunction at the hip joint.
planes. Interestingly, when separated into three age categories, variations between the youngest and oldest subjects were small and probably of little clinical significance with the exception of hip extension where ROM in the older subjects was over 20% less than that of the youngest (6).
 Figure 3.1. The ground reaction force (GRF) acts to adduct the hip joint. The muscles work to internally counteract the externally generated moment and keep the joint stable. Because of the smaller lever arm of the muscles compared to that of the ground reaction force, the muscles need to pull in excess of the GRF. The sum of both GRF and muscle force is balanced by the joint contact force, which typically reaches up to two and a half times the body weight during gait. |
Table 3.1 Motion and Peak Moments During Gait of Healthy Adultsa | ||||||||
|---|---|---|---|---|---|---|---|---|
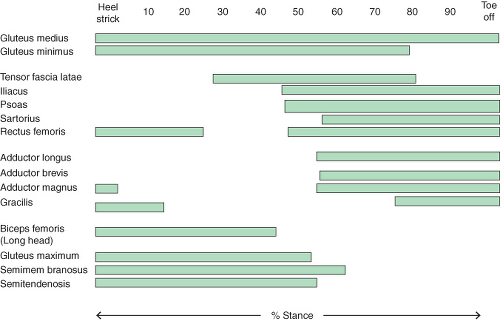
Forces at the Hip Joint The external moments measured in a gait laboratory are surrogate markers of the load experienced at the hip joint during ambulation. Actual forces at the hip must be either measured directly from implants instrumented with force transducers or estimated using analytical models with external moments and/or EMG as input. The measurement of hip forces is limited to subjects receiving implants (e.g., total hip or hemi-arthroplasties). Because it requires complex modifications of the implant to incorporate strain gauges, amplifiers, and telemetry (to avoid extruding cables), only data from a very limited number of arthroplasty patients is available. Rydell (19) published the first such work in 1966. The most complete data set is available from Bergmann et al., (20,21) who published data on five subjects. During level walking the force at the hip joint generally reaches an initial peak in early stance and a second peak in late stance (17,18). However, EMG can be easily used to determine which muscle is active during a particular period of the gait cycle and to what extent.
Forces at the Hip Joint The external moments measured in a gait laboratory are surrogate markers of the load experienced at the hip joint during ambulation. Actual forces at the hip must be either measured directly from implants instrumented with force transducers or estimated using analytical models with external moments and/or EMG as input. The measurement of hip forces is limited to subjects receiving implants (e.g., total hip or hemi-arthroplasties). Because it requires complex modifications of the implant to incorporate strain gauges, amplifiers, and telemetry (to avoid extruding cables), only data from a very limited number of arthroplasty patients is available. Rydell (19) published the first such work in 1966. The most complete data set is available from Bergmann et al., (20,21) who published data on five subjects. During level walking the force at the hip joint generally reaches an initial peak in early stance and a second peak in late stance (Fig. 3.4). These peaks are usually similar in magnitude; however, different muscles are active during these two phases of the gait cycle. The average peak load at the hip while walking at a “normal” speed is approximately 240% body weight (BW). This is slightly more than standing in single leg stance. When going upstairs the joint contact force is 250% BW and downstairs 260% BW. The peak contact forces during all other common daily activities are comparatively small, except for stumbling. Peak forces during unanticipated stumbling have been found as high as 870% BW (<A onclick="if (window.scroll_to_id) { scroll_to_id(event,'R22-3'); return false; }" onmouseover="window.s to handle (and thus more common) because it does not need an a priori knowledge of structure properties. All it needs is knowledge of the geometry of the involved structures and their displacement vectors over time.
Following the inverse dynamics approach and knowing the three-dimensional position of the limb segments and the ground reaction force, it is then assumed that the external forces and moments are balanced by a set of forces and moments acting internally, which are primarily generated by muscle contraction, other soft tissue tension and articular reaction forces. Because of the redundancy of the internal structures, this approach, however, induces more unknowns than can be solved with the number of equations available. In general, two attempts have been made to solve this indeterminate problem. The first reduterns as compared to age-matched control subjects (24,25
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|