Fig. 53.1
The preoperative x-ray plan sagittal scan of arthritic ankle evidences the presence of anterior bony spur both on talar and tibial side

Fig. 53.2
The postoperative x-ray plan sagittal scan of arthritic ankle, submitted to arthroscopic debridement, confirms the surgical result of bony spur removal on talar and tibial side, recreating a good anterior articular space
The ultrasound shows a high reliability because of the minimally invasive and big accuracy of the detected images, because it highlights not only the ligaments but also the associated tendon degenerative injuries. Magnetic resonance imaging provides the opportunity to study articular areas deeply, which escape the ultrasound examination and which are not detectable by traditional radiographs: its use in chronic condition is appropriate to particularly selected cases of low reliability with other instruments, both for appropriate treatment and for prognostic purposes.
53.5 Surgical Arthroscopic Procedure
Arthroscopy belongs indication for the first treatment of ankle arthritis, despite having gained over time its precise role in all the other joints as a tissue-saving procedure with lack of invasiveness. One of the first choice treatments is articular debridement performed by arthroscopy. Arthroscopy is addressed to evaluate the disorder (see Fig. 53.3), to remove synovial pathology, bone spurs, loose bodies (see Fig. 53.4), and ossicles that make symptomatic ankle joint as hindfoot [15, 16]. The reactive chondral debris-induced modifications of soft tissues are disabled with arthroscopic surgery. This treatment is limited to the initial ankle arthritis, without any deformity, any mechanical axis variation, and any joint space absence. Arthroscopy has the role of mini-invasive procedure and is respectful of disabling skin dystrophies as consequences of important traumas or bony profile deformity, thus avoiding the potential complications secondary to infection and to low capability of mortified skin to regenerate. It permits a selectivity of treatment to single sides of joint, not possible in open surgery because it is limited by surgical access, allowing to explore and to address surgery both anteriorly and posteriorly, laterally and medially, simply by exchanging the instruments inside the surgical portals, thus allowing wider angles of vision and work.
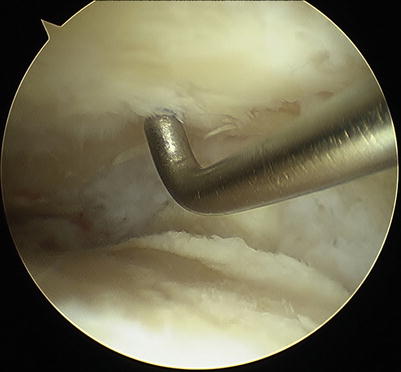

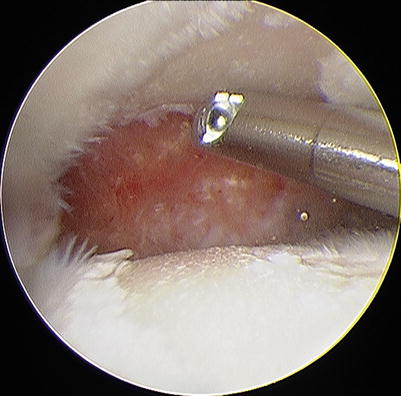
Fig. 53.3
The surgical picture shows the space between the two tibial (above) and talar (below) chondral surfaces: a big erosion of cartilaginous layer involves all the talar dome, while on tibial plafond, the detached cartilage is simply removed by probe which is going to appreciate the consistency of the articular several layers
Fig. 53.4
An ossicle is found at the malleolar tip after cleaning up the joint and removing all the pathological tissue which hides the distal medial compartment: the punch grip is grabbing it out from the articular space
The association of surgical debridement with articular distraction by external fixation is reserved to younger patients with severe arthritis at the final stage, who are arthroplasty or arthrodesis candidates. The association between arthrodesis and arthroscopy gave fresh impetus to this surgical choice, ensuring a very low local aggressiveness despite the total big bone removal from the joint necessary for a good articular fusion. Arthrodesis is the treatment indicated at final stage of osteoarthritis and at failure of all other therapies, within the correct indication. However, it is not indicated for athletes in full sports activity because of the total lack of motion, representing the end of any ankle sports-related performance.
The arthroscopic procedure longer used is articular debridement (see Fig. 53.5); the term debris comes from French language and is reused literally in English language [17]. It is considered as the remaining of biological tissue, bone or cartilage, physiological or not, loose inside the joint, or linked to articular structures, which can assume a pathological significance according to its quantity, its placement, and its presence in critical areas subjected to movement or friction. Its presence becomes symptomatic triggering a widespread articular suffering, which often is associated to chondral surface pathology [18]. With the diffusion of arthroscopic removal of those debris and fragments, debridement is stated as one of the most common ankle joint surgical procedures. Technique [15] provides the patient’s assessment supine with inferior limb on a leg holder and the ankle distracted, remaining free to perform movements on surgeon’s needs, despite firmly wrapped in a noninvasive traction. If the joint region to be treated is posterior, the patient is assessed in prone position, with foot outside the surgical bed on a roll pillow placed below the pretibial region, in order to release any movement of the joint from bed [16]. In this case, ankle traction is not needed, just forcing movements to open ankle joint enough to be addressed by instruments. Alternating the position of scope and instruments on three selected portals, a targeted removal of pathological inflamed and fibrotic tissues is performed: tools such as basket or radio-frequency wands are needed to remove particularly tough and stiff tissues which make blind any visualization. Once cleaned up the spotted compartment, those loose bodies or ossicles in released articular recesses or gutters can be highlighted. If chronic inflammatory clinical aspects are diffused inside compartments, the association with synovectomy remains indicated, as largest as possible both in medial and lateral and frontal and rear compartment, although final results remain fair in short to medium term because of the possibility of inflammatory tissue recurrence. These surgical procedures make valid the arthroscopic debridement in solving a big part of symptoms of athletes. The rehabilitation protocol is very fast, permitting an immediate weight-bearing with crutches if needed by the patient: exercise to reinforce strength and to develop proprioception is immediately started. Better coordination between muscle and training activities addressed to the perception of balance makes possible to prevent the occurrence of further trauma, resulting in improved muscle strength and improved proprioceptive response from the operated ankle.