Anatomy of Acetabulum
Michael Leunig
Carl R. Freeman
Reinhold Ganz
Martin Beck
The normal native hip is one of the most stable joints in the human body, but astonishingly it allows a wide range of motion. In addition, it has a profoundly effective lubrication mechanism which allows almost no wear despite a lifetime of around 100 million mechanical cycles. The acetabulum is the socket of the ball-and-socket hip joint. Although simplicity is suggested in its most basic understanding as a containing device for the femoral head, the acetabulum in reality is a complex and elegantly designed structure; together with the labrum it is responsible for both the high stability of the hip joint and the mechanics and lubrication of the articular surface. It is shaped and oriented in such a way as to allow wide ranges of motion in the planes most needed for human activities. Finally, the acetabulum has a wealth of vascular and nerve supply to allow it to meet the needs of vigorous human activity (Figs. 5.1 and 5.2) (1).
Development
The early development of the hip begins with the formation of the lower limb buds on the fourth week of embryologic development, and is practically complete by the 16th week (Fig. 5.3A–F) (2,3,4). Around the sixth week a highly cellular
structure forms in the proximal portion of the lower limb bud. This structure, a scleroblastema, includes a central, spherical portion composed of two distinct components. The inner component is a sphere densely packed with primitive chondroblasts which will differentiate to form the femoral head. The outer component is a surrounding “anlage” with three disk-shaped masses which will form the ilium, ischium, and pubis (2,3,4). The region of the future joint space becomes marked by a crescent of densely packed cells between these two regions. By the end of the eighth week, the blood supply
of the developing hip is fully established (2). From weeks 6 to 12, the hip increases in size via interstitial growth, and by the 12th week the joint space has formed via apoptosis of cells between the anlage and the femoral head. The ligamentum teres, or ligamentum capitis femoris, forms at this time in the region of the cotyloid notch (4). The limbus, which gives rise to the brim of the acetabulum and labrum, has also formed by this time. By the 16th week, the centers of ossification of the ilium, ischium, and pubis emerge, and the triradiate cartilage is formally created (Fig. 5.4A,B) (2,4). The hip enlarges during the remainder of fetal growth, but undergoes no other morphologic changes until infancy.
structure forms in the proximal portion of the lower limb bud. This structure, a scleroblastema, includes a central, spherical portion composed of two distinct components. The inner component is a sphere densely packed with primitive chondroblasts which will differentiate to form the femoral head. The outer component is a surrounding “anlage” with three disk-shaped masses which will form the ilium, ischium, and pubis (2,3,4). The region of the future joint space becomes marked by a crescent of densely packed cells between these two regions. By the end of the eighth week, the blood supply
of the developing hip is fully established (2). From weeks 6 to 12, the hip increases in size via interstitial growth, and by the 12th week the joint space has formed via apoptosis of cells between the anlage and the femoral head. The ligamentum teres, or ligamentum capitis femoris, forms at this time in the region of the cotyloid notch (4). The limbus, which gives rise to the brim of the acetabulum and labrum, has also formed by this time. By the 16th week, the centers of ossification of the ilium, ischium, and pubis emerge, and the triradiate cartilage is formally created (Fig. 5.4A,B) (2,4). The hip enlarges during the remainder of fetal growth, but undergoes no other morphologic changes until infancy.
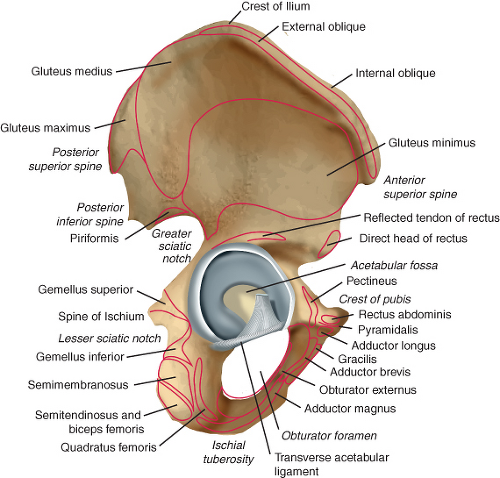 Figure 5.1. A lateral view of the hemipelvis and acetabulum. |
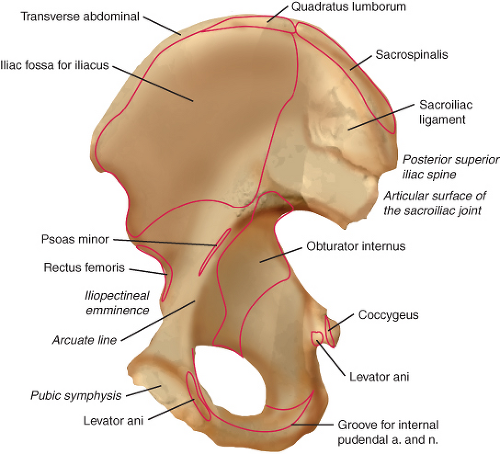 Figure 5.2. A medial view of the hemipelvis. |
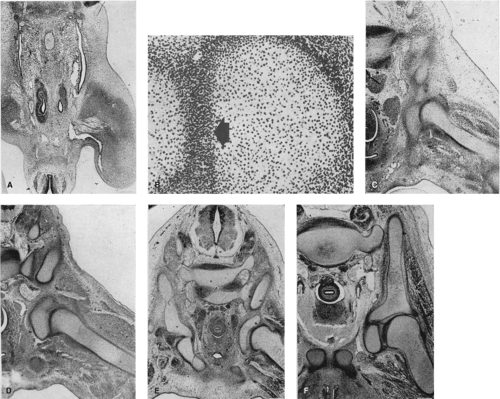 Figure 5.3. A: Around the sixth week, the hip begins to form as a densely packed group of cells called a scleroblastema, from which forms the anlage and the femoral head. B: The region of the future joint space is marked by a crescent of densely packed cells (arrow head) which will eventually undergo apoptosis to form a joint space, and formally separate the acetabulum from the head. C–E: From weeks 6 to 12 the anlage and femoral head increase in size via interstitial growth, and the joint space forms. F: By the 12th week, the hip has formed the following: a joint space, the ligamentum teres, the cotyloid fossa, and the limbus. (Reprinted with permission from Strayer LM. The embryology of the human hip joint. Yale J Biol Med. 1943;16:13–26.6.) |
The acetabulum and labrum develop much of their final morphologic features during infancy and childhood (5,6). Eventually formed as a coalescence of the three innominate bones of the pelvis, the hip is entirely cartilaginous at birth and remains so during much of the first year. Between the innominate bones lies a cartilaginous T-shaped structure (Fig. 5.5A,B) (6). This structure, the triradiate cartilage, is responsible for the formation of the anterior wall, posterior wall, and the dome of the acetabulum. It is the triradiate cartilage that is most responsible for the final depth of the acetabulum (6). Laterally, the triradiate cartilage gives rise to a circumferential lip composed of hyaline cartilage centrally and fibrocartilage on the periphery. This cartilaginous cup is the structure that will form the majority of the mature acetabulum when growth is complete, and is the location where the acetabular epiphyses form, all under the constantly shaping stimulus of the femoral head. The ilium and ischium contribute significantly to the final morphology of the dome and the
posterior wall of the hip, respectively. In contrast, the pubis contributes very little to the final structure of the mature acetabulum. This is because the anterior wall is almost completely formed by the os acetabuli, an epiphysis that forms adjacent to the pubis (Fig. 5.6) (6). The os acetabuli form after age 7 and have completed growth and closed before age 9 (6). The triradiate cartilage closes at age 14 to 16, but the acetabular epiphyses can remain open as late as 18 years (7).
posterior wall of the hip, respectively. In contrast, the pubis contributes very little to the final structure of the mature acetabulum. This is because the anterior wall is almost completely formed by the os acetabuli, an epiphysis that forms adjacent to the pubis (Fig. 5.6) (6). The os acetabuli form after age 7 and have completed growth and closed before age 9 (6). The triradiate cartilage closes at age 14 to 16, but the acetabular epiphyses can remain open as late as 18 years (7).
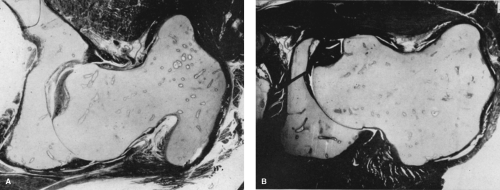 Figure 5.4. Photomicrograph of a fetal hip at about 16 weeks. All the structures of the hip have formed and the hip is entirely cartilaginous (4). By the 16th week, the centers of ossification of the ilium, ischium, and pubis emerge, and the triradiate cartilage is formally created. A: A cross section through the center of the hip shows the femoral head, acetabulum, the anterior labrum, and the posterior labrum. B: A cross section of the caudal portion of the hip includes the ligamentum teres. (Reprinted with permission from Cashin M, Uhthoff H, O’Neill M, et al. Embryology of the acetabular labral-chondral complex. J Bone Joint Surg Br. 2008;90:1019–1024.) |
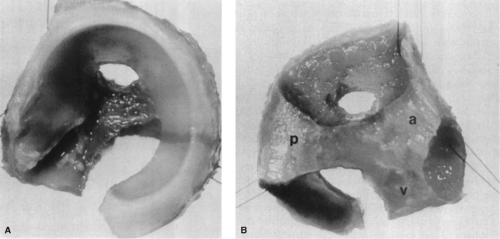 Figure 5.5. Normal acetabular cartilage complex of a 1-day-old infant. The ilium, ischium, and pubis have been removed with a curette. A: The lateral view shows the cup-shaped acetabulum. B: The medial view shows the three flanges of the triradiate cartilage. The anterior flange (a) is located between the ilium and pubis and is slanted superiorly; the posterior flange (p) is horizontal and is located between the ilium and ischium; and the vertical flange (v) is located between the pubis and ischium. (Reprinted with permission from Ponseti IV. Growth and development of the acetabulum in the normal child. Anatomical, histological, and roentgenographic studies. J Bone Joint Surg Am. 1978;60:575–585.) |
Landmarks
Surrounding the adult acetabulum are several boney landmarks that can be used internally and externally as a guide for the position of the native anatomy. The primary landmark of the hip and acetabulum is the anterior superior iliac spine (ASIS). This landmark lies superior and just lateral to the acetabulum in the coronal plane. It has been called the lighthouse of the hip because of its prominence, and it can be easily palpated, even on obese patients, making it an ideal anterior landmark for the hip. It is used to determine the location of the anterior column, the anterior wall, and the iliac crest. The lateral femoral cutaneous nerve crosses the inguinal ligament 1.4 to 2.4 cm medial to the ASIS. It then proceeds to cross the lateral border of the sartorius muscle 6 cm inferior to the ASIS (8). Another landmark, the anterior inferior iliac spine, which is one fingerbreadth inferior to the ASIS, lies directly anterior and superior to the acetabulum. The iliopectineal eminence, a residual of the pubic extension of the triradiate cartilage, is an important internal landmark marking both the medial border of the acetabulum in the coronal plane (Fig. 5.7) (9) and the iliopectineal bursa. It is an essential landmark to note when performing a
periacetabular osteotomy. Finally, the infracotyloid notch, which is a notch on the posterior ischium, just posterosuperior to the ischial tuberosity and hamstring origin is an internal landmark. It denotes an area of bone adjacent to the inferior acetabular rim, and is used as a guide when performing periacetabular osteotomy. The ischial spine is a radiologic landmark. Its spur like appearance is formed by the sacrospinous ligament and separates the greater and lesser sciatic notch. When visible on orthograde anteroposterior radiographs of the pelvis it may indicate retroversion of the acetabulum (10).
periacetabular osteotomy. Finally, the infracotyloid notch, which is a notch on the posterior ischium, just posterosuperior to the ischial tuberosity and hamstring origin is an internal landmark. It denotes an area of bone adjacent to the inferior acetabular rim, and is used as a guide when performing periacetabular osteotomy. The ischial spine is a radiologic landmark. Its spur like appearance is formed by the sacrospinous ligament and separates the greater and lesser sciatic notch. When visible on orthograde anteroposterior radiographs of the pelvis it may indicate retroversion of the acetabulum (10).
 Figure 5.6. The area of cross section defined by the box labeled 1 represents the anterior wall, an area of the acetabulum formed only by contributions of the acetabular epiphysis which forms within the anlage (a structure extending outward from the triradiate cartilage) and the os acetabuli epiphysis, with almost no contribution of the pubic bone. However, the box labeled 2 shows the acetabular dome, a region of the acetabulum formed by contributions from both the cartilage anlage and the ossification center of the ilium. (Redrawn from Ponseti IV. Growth and development of the acetabulum in the normal child. Anatomical, histological, and roentgenographic studies. J Bone Joint Surg Am. 1978;60:575–585.) |
 Figure 5.7. The iliopectineal eminence lies directly anterior to the inferior portion of the anterior wall of the acetabulum. (Reprinted with permission from Govsa F, Ozer MA, Ozgur Z. Morphologic features of the acetabulum. Arch Orthop Trauma Surg. 2005;125:453–461.) |
Osteology
The bony acetabulum, formed by the confluence of the ilium, ischium, and the pubis, forms a concentric dome over the femoral head. Its coverage of the femoral head, less than a hemisphere, is approximately 170 degrees (11). The male acetabulum is deeper than the female on average, but the female acetabular fossa is deeper (11). The average diameter of the native acetabulum is 52 ± 4 mm, with females having smaller diameter than males on average (Table 5.1) (11,12,13,14,15,16,17,18,19).
It has become common convention to refer to points around the lateral acetabulum and labrum as positions on a clock face (Fig. 5.8) (11). Using this nomenclature, 6:00 refers to the midpoint of the fossa inferiorly, and 12:00 refers to the superior part of the acetabulum directly across from the midpoint of the fossa. The 3:00 position refers to the anterior acetabulum on both right and left hips, and the 9:00 position refers to the midpoint of the posterior wall on both left and right hips. Four major regions of the bony acetabulum contribute to coverage of the femoral head: the anterior wall, the posterior wall, the medial wall, and the dome or tectum (Latin for roof). The anterior wall is directly connected to the pubis, and the superior pubic ramus extends anteriorly from its medial border. The anterior wall and anterior rim of the acetabulum have a variable morphology. Most acetabula have a prominence that extends from the anterior rim from about 12:30 to 3:00 (Fig. 5.8) (11). Proceeding medially along the anterior wall, there is an indentation in the anterior wall adjacent to a prominent groove on the pelvic rim. This groove, just lateral to the iliopectineal eminence, provides a track for the iliopsoas, and represents the most medial aspect of the anterior wall easily accessible with an arthroscope.
Although a wide range of possibilities exists in regard to configurations of the anterior wall, four are most common (9). These are curved (60%), angular (25.5%), straight (4.5%), and irregular (9.5%) (Fig. 5.9). The iliopectineal eminence lies just anterior to the inferior half of the anterior wall on the pubic brim (Fig. 5.7). Thus, it is an important landmark representing the anterior and medial boundaries of the joint.
The posterior wall is larger and projects more laterally than the anterior wall. Its lateral edge has a nearly vertical but slightly curved route, with few prominences or grooves, and little variation between individuals (9,20). The posterior wall is a major bony contributor to the stability of the hip. Trauma research has shown that hip stability depends most on an intact posterior wall, and to lesser extent on the capsule being intact (21). In a cadaver study, 100% of hips were stable with as much as 25% of posterior wall disrupted, but with 33% of the posterior wall disrupted only 75% of hips
were stable. When 50% of the posterior wall was disrupted all specimens were found to be unstable (21).
were stable. When 50% of the posterior wall was disrupted all specimens were found to be unstable (21).
Table 5.1 Comparison of Hip Diameter Values from the Literature | |||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||
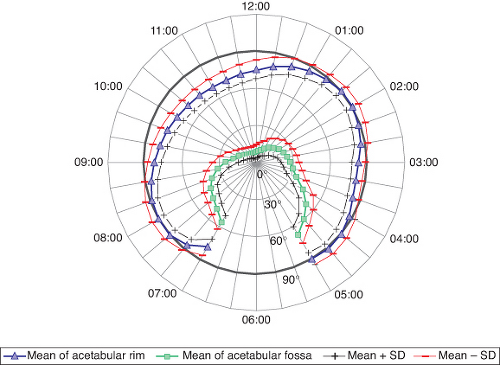 Figure 5.8. This figure shows mean and standard deviation of rim and fossa values as a function of its geographic reconstruction. Zero degree is at the pole of the acetabular hemisphere; 30, 60, and 90 degrees are indicating the depth of the cup (latitude). The circle at 90 degrees marks the equatorial level of the hemisphere. The rim, fossa, and articular surface locations are indicated in a clockwise distribution, with the acetabular notch as the caudal landmark for 6:00 (longitude). The 3:00 position represents a point directly anterior on the anterior wall in both right and left hips. The three prominent areas are anterosuperior, anteroinferior, and posteroinferior. The two depressions along the anterior and posterosuperior walls can clearly be distinguished. (Modified from Köhnlein W, Ganz R, Impellizzeri FM, et al. Acetabular morphology: Implications for joint-preserving surgery. Clin Orthop Relat Res. 2009;467:682–691.) |
Related posts:
 Diagnostic Categories and Definitions for the Adult Hip
Measurement of Treatment Outcomes in the Young Patient with a Hip Disorder
Hip Arthroscopy Anatomy and Access to the Central Compartment
Chiari and Salvage Osteotomy for the Treatment of Symptomatic Acetabular Dysplasia
FAI: Extra-articular Bony Impingement
Treatment of Slipped Capital Femoral Epiphysis Deformities in Skeletally Mature Patients
Diagnostic Categories and Definitions for the Adult Hip
Measurement of Treatment Outcomes in the Young Patient with a Hip Disorder
Hip Arthroscopy Anatomy and Access to the Central Compartment
Chiari and Salvage Osteotomy for the Treatment of Symptomatic Acetabular Dysplasia
FAI: Extra-articular Bony Impingement
Treatment of Slipped Capital Femoral Epiphysis Deformities in Skeletally Mature Patients
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


