Chapter 17 Amputations of the Hip and Pelvis
Disarticulation of the Hip
Anatomical Hip Disarticulation
 With the patient in the lateral decubitus position, make an anterior racquet-shaped incision (Fig. 17-1A), beginning the incision at the anterior superior iliac spine and curving it distally and medially almost parallel with the inguinal ligament to a point on the medial aspect of the thigh 5 cm distal to the origin of the adductor muscles. Isolate and ligate the femoral artery and vein, and divide the femoral nerve; continue the incision around the posterior aspect of the thigh about 5 cm distal to the ischial tuberosity and along the lateral aspect of the thigh about 8 cm distal to the base of the greater trochanter. From this point, curve the incision proximally to join the beginning of the incision just inferior to the anterior superior iliac spine.
With the patient in the lateral decubitus position, make an anterior racquet-shaped incision (Fig. 17-1A), beginning the incision at the anterior superior iliac spine and curving it distally and medially almost parallel with the inguinal ligament to a point on the medial aspect of the thigh 5 cm distal to the origin of the adductor muscles. Isolate and ligate the femoral artery and vein, and divide the femoral nerve; continue the incision around the posterior aspect of the thigh about 5 cm distal to the ischial tuberosity and along the lateral aspect of the thigh about 8 cm distal to the base of the greater trochanter. From this point, curve the incision proximally to join the beginning of the incision just inferior to the anterior superior iliac spine.

 Divide the pectineus about 0.6 cm from the pubis.
Divide the pectineus about 0.6 cm from the pubis.





 Identify, ligate, and divide the sciatic nerve.
Identify, ligate, and divide the sciatic nerve.

 Incise the hip joint capsule and the ligamentum teres to complete the disarticulation (Fig. 17-1B).
Incise the hip joint capsule and the ligamentum teres to complete the disarticulation (Fig. 17-1B).


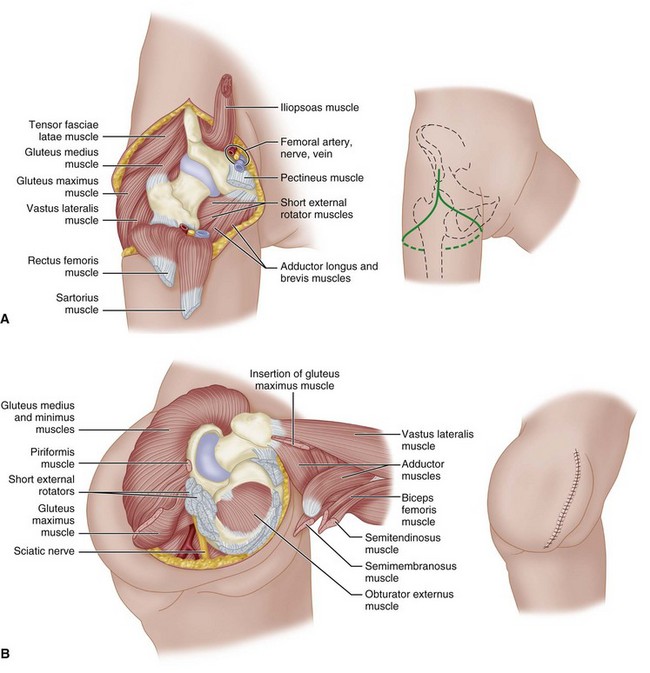
FIGURE 17-1 Boyd disarticulation of hip. A, Femoral vessels and nerve have been ligated, and sartorius, rectus femoris, pectineus, and iliopsoas muscles have been detached. Inset, Line of skin incision. B, Gluteal muscles have been separated from insertions, sciatic nerve and short external rotators have been divided, and hamstring muscles have been detached from ischial tuberosity. Inset, Final closure of stump. SEE TECHNIQUE 17-1.
(Redrawn from Boyd HB: Anatomic disarticulation of the hip, Surg Gynecol Obstet 84:346, 1947.)
Posterior Flap
 Begin the incision at the level of the inguinal ligament, carry it distally over the femoral artery for 10 cm, curve it along the medial aspect of the thigh, continue it laterally and proximally over the greater trochanter, and swing it anteriorly to the starting point. A posteromedial flap long enough to cover the end of the stump is formed.
Begin the incision at the level of the inguinal ligament, carry it distally over the femoral artery for 10 cm, curve it along the medial aspect of the thigh, continue it laterally and proximally over the greater trochanter, and swing it anteriorly to the starting point. A posteromedial flap long enough to cover the end of the stump is formed.

 Abduct the thigh widely, and divide the adductor muscles at their pubic origins.
Abduct the thigh widely, and divide the adductor muscles at their pubic origins.
 Section the two branches of the obturator nerve so that they retract away from pressure areas.
Section the two branches of the obturator nerve so that they retract away from pressure areas.

 Identify, ligate, and divide the sciatic nerve.
Identify, ligate, and divide the sciatic nerve.
 Divide the joint capsule, and complete the disarticulation.
Divide the joint capsule, and complete the disarticulation.

Hemipelvectomy
The standard hemipelvectomy employs a posterior or gluteal flap and disarticulates the symphysis pubis and sacroiliac joint and the ipsilateral limb. An extended hemipelvectomy includes resection of adjacent musculoskeletal structures, such as the sacrum or parts of the lumbar spine. In a conservative hemipelvectomy, the bony section divides the ilium above the acetabulum, preserving the crest of the ilium. Internal hemipelvectomy is a limb-sparing resection, often achieving proximal and medial margins equal to the corresponding amputation. This procedure is discussed in Chapter 24.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


