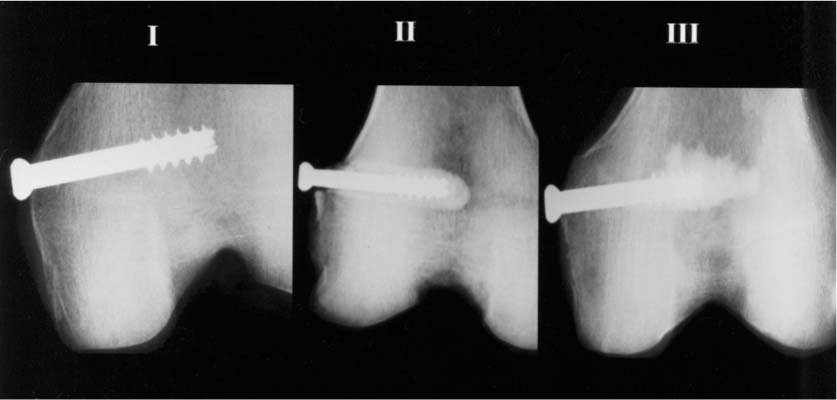
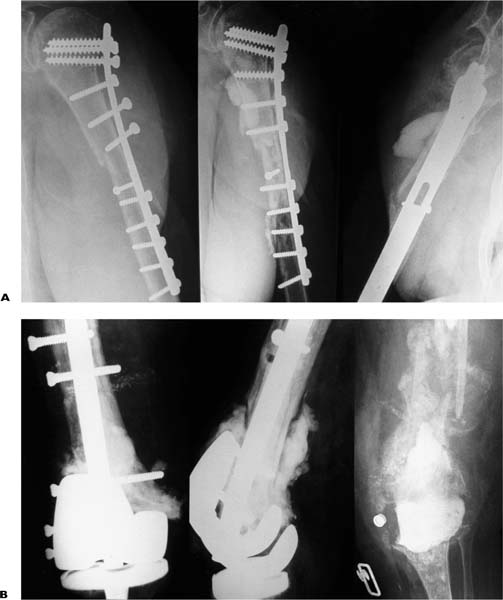
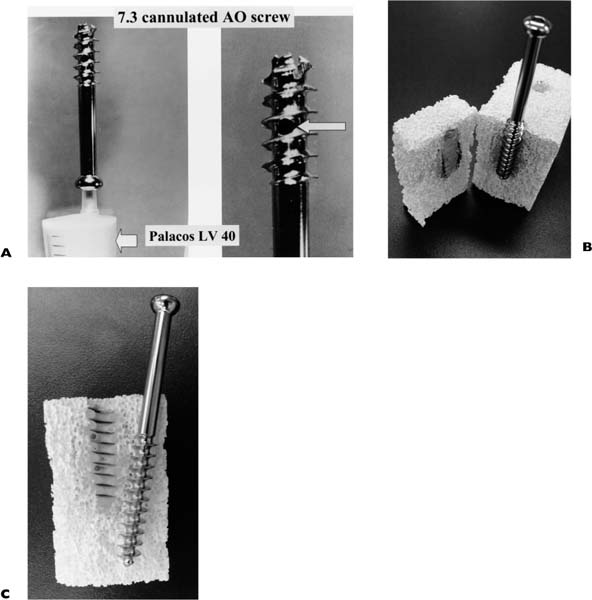
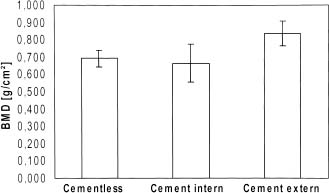
Chapter 22 The structure of our society in the coming decades will include a higher number of elderly people, which will increase the consumption of a substantial proportion of the health care resources.1,2 Although recent research suggests that the incidence of osteoporotic fractures has experienced either a leveling off or a slight downturn in North America and Europe, the number of patients with osteoporotic fractures will continue to rise in all continents, as a result of aging.3–6 New implant and surgical techniques need to be developed to improve treatment and allow rapid rehabilitation for the patient.7–10 When bone quality is impaired and stable fracture fixation is impossible, augmentation of the osteosynthesis is advocated. For fixation of screws, cement based on polymethylmethacrylate (PMMA)11–14 or ceramics and resins15 has been used with success. The use of plates for the treatment of osteoporotic fractures is often problematic as the purchase of screws in the bone is reduced and the precarious soft tissue situation makes surgical dissection impossible. Another option to overcome these problems is the use of oversized plates that span the fracture over a long distance.16 Another approach to improve stability of a plate osteosynthesis is the application of an intramedullary rod made of resorbable polymers that produces adequate purchase for screws.8,10,17 To prevent the detrimental effects of PMMA injected in the fracture site12,18 we investigated the usefulness of PMMA, injected through side holes situated in the threaded portion of a modified cannulated 7.3 mm AO screw (Mathys, Belgium) to enhance the purchase of these screws in the epimetaphyseal region of long bones (Figs. 22–1A,B). The “cement screw” is a partially cannulated, self-drilling, and self-tapping 7.3 mm AO screw with a thread length of 32 mm. The screw is made of implant-quality stainless 316L steel. The top of the cannulated screw is closed by insertion of a press-fit metal plug. In the threaded portion, three side holes of 2 mm are drilled. Through these side holes the injected cement (Palacos LV 40, Shering-Plough, Brussels Belgium) can flow sideways into the cancellous bone, surrounding the threaded portion of the screw (Figs. 22–2A,B,C). Bending test was used to evaluate the modified cement screw versus the regular cannulated screw. Two groups of four screws were loaded in a three-point fixture. The support distance was 40 mm. The force was applied via a steel roller of 8.3 mm diameter and was applied at a test velocity of 1 mm/min. Pullout test was used to evaluate the pullout strength of both screw types. Fifteen cold-preserved distal human femurs were selected from a pool of 60 fresh-frozen bones (Fig. 22–3). The surrounding soft tissue was removed, and the bones were wrapped in moist cloths impregnated with 6% glutaraldehyde, put in a watertight container, and stored at –40°C until thawed 24 hours prior to testing. For mechanical testing, the femurs were sawed through, 15 cm above the proximal end of the incisura femoris. For easy handling in the testing machine, the sawed-off portion was placed in a steel pot and embedded in PMMA. The osteoporotic state was evaluated with a computed imaging tomograph (Hologic QDR4500A). Only bones with a mean density below 1 g/cm3 were used. FIGURE 22–1 (A) Loosening of a plate osteosynthesis in a 67-year-old male, 4 months after surgery. Revision of the osteosynthesis was done using large amounts of bone cement. The bone cement is protruding into the fracture site, preventing the sound healing of the fracture. (B) An example of the detrimental effect of bone cement injected into the fracture site. This 70-year-old female had a fracture above her knee prosthesis. The retrograde nail was reinforced with bone cement with the undesirable presence of bone cement in the fracture and surrounding tissue. The fracture did not heal and became infected, necessitating a resection arthroplasty. The 15 specimens were divided randomly into three groups each consisting of five femora (Fig. 22–4). • Group I, cannulated screw (65 mm length and 32 mm threaded length) inserted in the lateral epicondyle at right angles to the shaft and the frontal plane of both condyles. The screw head was left 3 mm from the cortex, so that the clamp of the servohydraulic testing machine could be fitted for pullout testing. FIGURE 22–2 (A) The modified 7.3 mm cannulated screw. (Reprinted with permission from Broos PL, Robijns FM. Fractures of the distal femur. In: Obrant K, ed. Management of Fractures in Severely Osteoporotic Bone. London: Springer; 2000:280–293.) (B) Injection of Palacos LV 40 through the ported screw in a block made of calcium sulphate. (C) Magnification of the section through the cement plug, showing the flow of the cement into the porous material. FIGURE 22–3 Example of cadaveric femora after insertion of a cannulated 7.3 mm screw (group I), insertion of a cannulated screw in a plug of bone cement (group II), and insertion of the modified cannulated screw (group III). FIGURE 22–4 Bone mineral density of the three groups of cadaveric bone. • Group II, ported screws of the same length inserted in the same manner. After screw insertion 5 cc of liquid cement was injected with a medical plastic syringe (Braun®, Germany) through the head of the screw. • Group III, cannulated screw of the same dimensions as the previous ones, potted in a cylinder of PMMA (15 × 80 mm). This cylinder was created by a metal punch with a diameter of 15 mm. The cement was allowed to harden for 2 days. Pullout force was measured by a load cell having a capacity of 30 kN (Model 2511–317, Instron Corp., Canton, MA) at a constant crosshead speed of 5 mm/min. The maximum force was determined for each test and defined as the pullout test. Starting in February 1998, we used these screws to reinforce plate osteosynthesis in 63 patients with 70 nonpathological fractures (45 subcapital humerus fractures, 5 distal femur fractures, 13 tibial fractures, 3 os calcis, and 4 ankle fractures) (Figs. 22–5A through D
ACEMENT SCREW FOR FIXATION IN
OSTEOPOROTIC METAPHYSEAL
BONE
THE SCREW DESIGN AND TESTING
IMPLANT DESIGN AND TESTING
PROSPECTIVE CLINICAL STUDY
Related posts:
 External Fixation in Osteoporotic Bone
External Fixation in Osteoporotic Bone
 Internal Fixation of Osteoporotic Acetabular and Pelvic Fractures
Internal Fixation of Osteoporotic Acetabular and Pelvic Fractures
 An Axially Mobile Plate for Fracture Fixation
An Axially Mobile Plate for Fracture Fixation
 The Huckstep Nail for Fixation of Mechanically Deficient Femoral Bone
The Huckstep Nail for Fixation of Mechanically Deficient Femoral Bone
 A Self-Guided Pedicle Screw for Anterior Fixation of Cervical Spine
A Self-Guided Pedicle Screw for Anterior Fixation of Cervical Spine
 Minimally Invasive Surgery for the Treatment of Vertebral Compression Fractures
Minimally Invasive Surgery for the Treatment of Vertebral Compression Fractures
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


