• The radius is typically entered proximal to the distal radial physis, and the nail should stop prior to touching the proximal radial physis. • The ulna is typically entered distal to the olecranon apophysis, and the nail stops prior to touching the distal ulnar physis.
Forearm Fractures
Intramedullary Rodding
Indications
 Intramedullary nails are designed for long-bone shaft (diaphyseal) fractures:
Intramedullary nails are designed for long-bone shaft (diaphyseal) fractures:
Examination/Imaging
 Deformity and swelling of the forearm typically indicate fracture location.
Deformity and swelling of the forearm typically indicate fracture location.
 Neurovascular examination is important prior to and after any manipulation.
Neurovascular examination is important prior to and after any manipulation.
 The skin should be examined for any abrasions or open areas.
The skin should be examined for any abrasions or open areas.
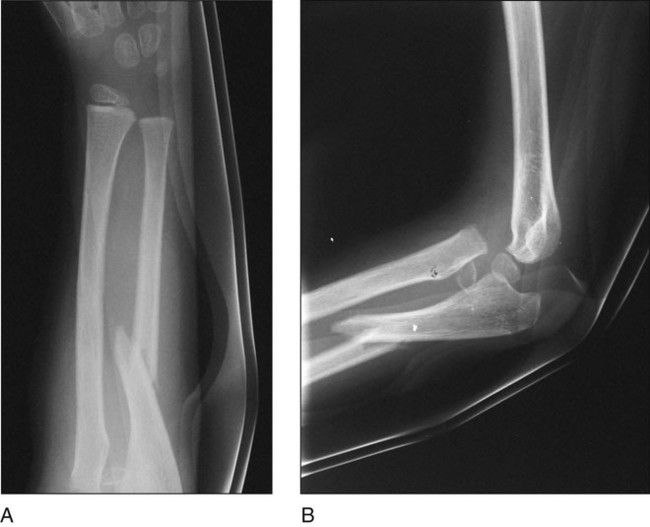
 Standard radiographs include anteroposterior and lateral views of the forearm and dedicated views of the wrist (Fig. 1A) and/or elbow (Fig. 1B) to rule out proximal or distal radioulnar joint dislocation above or below the fracture that can be associated with diaphyseal fractures.
Standard radiographs include anteroposterior and lateral views of the forearm and dedicated views of the wrist (Fig. 1A) and/or elbow (Fig. 1B) to rule out proximal or distal radioulnar joint dislocation above or below the fracture that can be associated with diaphyseal fractures.
Surgical Anatomy
 The physes need to be localized so that the intramedullary nails do not damage the growth cartilage.
The physes need to be localized so that the intramedullary nails do not damage the growth cartilage.
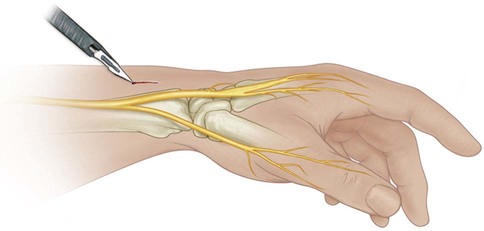
 Several branches of the superficial branch of the radial nerve traverse the dorsal radial aspect of the distal forearm and are often encountered when making the incision for the radial nail(Fig. 2). These branches need to be protected during the procedure to avoid creating an area of numbness distal to the incision.
Several branches of the superficial branch of the radial nerve traverse the dorsal radial aspect of the distal forearm and are often encountered when making the incision for the radial nail(Fig. 2). These branches need to be protected during the procedure to avoid creating an area of numbness distal to the incision.
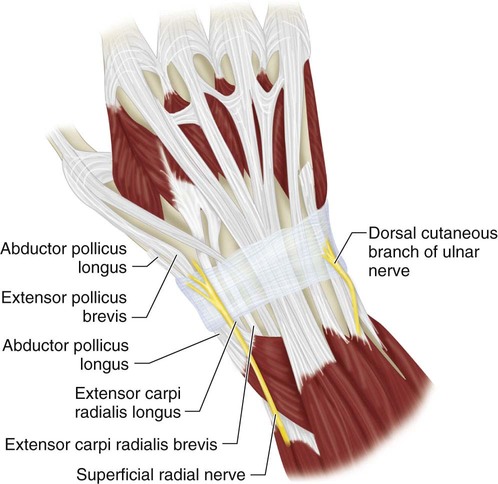
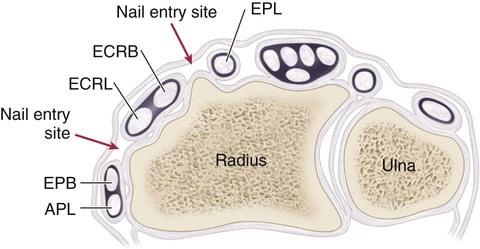
 The tendons on the radial aspect of the wrist at the level of incision (from radial to ulnar) are the abductor pollicis longus (APL), extensor pollicis brevis (EPB), extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), and extensor pollicis longus (EPL). Figure 3 shows the tendons and appropriate intervals for nail insertion at the distal radius.
The tendons on the radial aspect of the wrist at the level of incision (from radial to ulnar) are the abductor pollicis longus (APL), extensor pollicis brevis (EPB), extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), and extensor pollicis longus (EPL). Figure 3 shows the tendons and appropriate intervals for nail insertion at the distal radius.
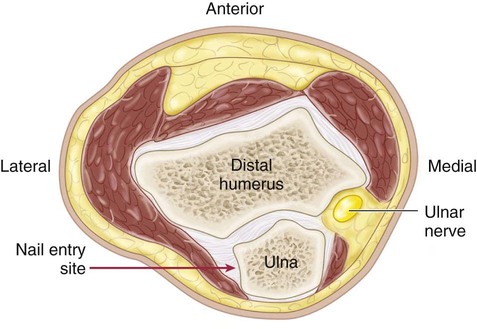
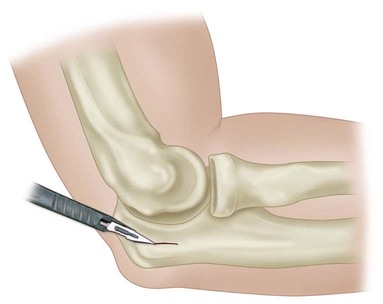
 The ulnar nerve is medial to the olecranon, so nail entry should always be on the lateral side of the olecranon to avoid ulnar nerve injury (Fig. 4).
The ulnar nerve is medial to the olecranon, so nail entry should always be on the lateral side of the olecranon to avoid ulnar nerve injury (Fig. 4).
Portals/Exposures
Radius
 A small incision is made on the dorsal radial aspect of the wrist just proximal to the physis (Fig. 6). Care is taken to protect the superficial branches of the radial nerve.
A small incision is made on the dorsal radial aspect of the wrist just proximal to the physis (Fig. 6). Care is taken to protect the superficial branches of the radial nerve.
 A proximal starting point should not be used for the radius.
A proximal starting point should not be used for the radius.
Ulna
 A small incision is made on the lateral aspect of the olecranon midway between the ulnohumeral joint and the posterior aspect of the olecranon and approximately 2 cm from the tip of the olecranon (Fig. 7).
A small incision is made on the lateral aspect of the olecranon midway between the ulnohumeral joint and the posterior aspect of the olecranon and approximately 2 cm from the tip of the olecranon (Fig. 7).
Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 32: Patellar Instability: Lateral Release and Medial Plication
32: Patellar Instability: Lateral Release and Medial Plication
![]() 18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


9: Forearm Fractures: Intramedullary Rodding