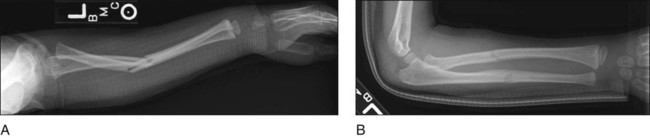
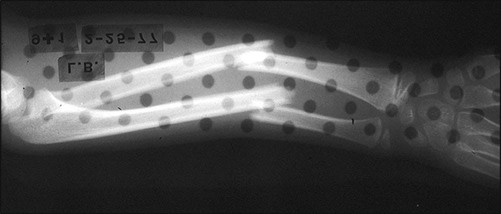
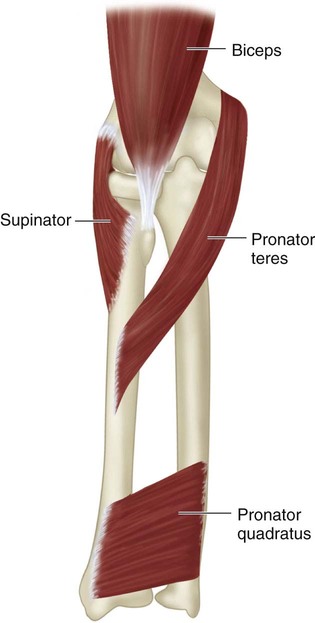
Figure 7 redrawn from Evans E. Fractures of the radius and ulna. J Bone Joint Surg [Br]. 1951;33:548–61. • Figure 1 shows AP (Fig. 1A) and lateral (Fig. 1B) radiographs of a volar-angulated forearm fracture (Case 1). Note the volar apex of the deformity with a nondisplaced fracture of the radius and ulna. The proximal radius crosses the ulna on the AP radiograph, suggesting pronation of the proximal fragment, although there is no true malrotation of the radius. • Figure 2 shows the initial radiograph of a displaced and angulated midshaft fracture of the radius and ulna in a 9-year-old girl (Case 2). • When both bones are fractured at the same level, there may be angular deformity without malrotation. • There may be pronation or supination deformity when the fractures are at different levels in the diaphysis. • Volar bowing is associated with supination of the distal fragment relative to the proximal fragment (Fig. 5A). Note that the proximal forearm is in a pronated position, but the distal forearm is in a neutral position. This indicates 90° torsional deformity in addition to the volar angulation. • Dorsal bowing is associated with pronation deformity of the distal fragment relative to the proximal fragment (Fig. 5B). Note that the proximal forearm is in a supinated position, but the distal forearm is in neutral. This indicates 90° torsional deformity in addition to the dorsal angulation. • Figure 6 shows the anatomy of the principal muscles affecting proximal fragment position for displaced fractures of the radius. • Proximal fractures of the radius rest in supination due to the unopposed action of the biceps and supinator muscles. • Midshaft fractures of the radius rest in neutral rotation because the pronator teres opposes the supinator and biceps while moving the radius toward the ulna as expected in the neutral pronation-supination position. • Countertraction is applied through a sling around the arm.
Forearm Fractures
Closed Treatment
Examination/Imaging
 Anteroposterior (AP) and lateral radiographs of the forearm should be made perpendicular to the distal humerus regardless of forearm pronation or supination.
Anteroposterior (AP) and lateral radiographs of the forearm should be made perpendicular to the distal humerus regardless of forearm pronation or supination.
Surgical Anatomy
 Figure 3A shows the normal shape of the radius. Note that the apex of the radial bow is lateral in supination. The radial tuberosity and the styloid are seen approximately on opposite sides of the radius.
Figure 3A shows the normal shape of the radius. Note that the apex of the radial bow is lateral in supination. The radial tuberosity and the styloid are seen approximately on opposite sides of the radius.

 Figure 3B shows the normal shape of the ulna. Note the varus bow of the proximal ulna. A line down the shaft passes through the lateral aspect of the olecranon. The coronoid and styloid can be used to judge rotation in older children and adults.
Figure 3B shows the normal shape of the ulna. Note the varus bow of the proximal ulna. A line down the shaft passes through the lateral aspect of the olecranon. The coronoid and styloid can be used to judge rotation in older children and adults.
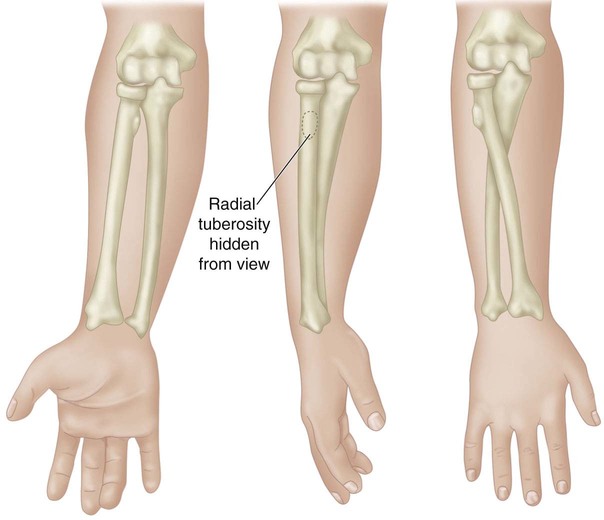
 Figure 4 illustrates the position of the proximal and distal forearm in various degrees of pronation or supination. Note that the radial tuberosity is approximately opposite the radial styloid and therefore opposite the position of the thumb. Also note that the proximal radius does not cross the proximal ulna when resting in a supinated position.
Figure 4 illustrates the position of the proximal and distal forearm in various degrees of pronation or supination. Note that the radial tuberosity is approximately opposite the radial styloid and therefore opposite the position of the thumb. Also note that the proximal radius does not cross the proximal ulna when resting in a supinated position.

Positioning
 Greenstick and nondisplaced fractures are reduced without any special positioning.
Greenstick and nondisplaced fractures are reduced without any special positioning.
Related posts:
 4: Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer
29: Epiphysiodesis of the Distal Femur/Proximal Tibia-Fibula
28: Femur Fracture: Closed Reduction and Spica Cast
46: Resection of Talocalcaneal Tarsal Coalition and Fat Autograft Interposition
57: Scoliosis Correction
10: Digital Syndactyly Release
4: Open Reduction and Internal Fixation of Displaced Medial Epicondyle Fracture Using a Screw and Washer
29: Epiphysiodesis of the Distal Femur/Proximal Tibia-Fibula
28: Femur Fracture: Closed Reduction and Spica Cast
46: Resection of Talocalcaneal Tarsal Coalition and Fat Autograft Interposition
57: Scoliosis Correction
10: Digital Syndactyly Release
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


7: Forearm Fractures: Closed Treatment














