• The abdomen must be kept free, and bolsters are placed at the chest and iliac crest regions. • The arms are flexed at the elbows and placed forward with the axilla remaining free of any compression. • The head needs to be placed in a standard headrest with access at the cervicothoracic junction.
Posterior Surgical Treatment for Scheuermann’s Kyphosis
Examination/Imaging
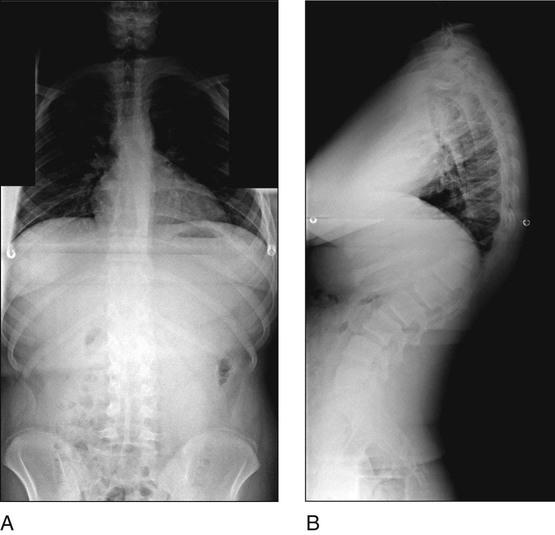
 Standing posteroanterior (PA) and lateral 36-inch radiographs are obtained. Figure 1 shows standing radiographs of a patient with kyphosis in PA (Fig. 1A) and lateral (Fig. 1B) views.
Standing posteroanterior (PA) and lateral 36-inch radiographs are obtained. Figure 1 shows standing radiographs of a patient with kyphosis in PA (Fig. 1A) and lateral (Fig. 1B) views.
 A lateral radiograph in hyperextesion with a bolster under the kyphotic apex is also obtained.
A lateral radiograph in hyperextesion with a bolster under the kyphotic apex is also obtained.
 Magnetic resonance imaging is done to assess for any possible thoracic disk herniations.
Magnetic resonance imaging is done to assess for any possible thoracic disk herniations.
Positioning
 The patient may be placed prone on a standard radiolucent spinal operating frame.
The patient may be placed prone on a standard radiolucent spinal operating frame.
 The patient must have appropriate somatosensory and motor evoked potential monitoring in place.
The patient must have appropriate somatosensory and motor evoked potential monitoring in place.
Procedure
Step 1
 Pedicle screw placement begins distally in the lumbar spine, taking care to include the lumbar vertebra that is centered over the sacral spine in the lateral view.
Pedicle screw placement begins distally in the lumbar spine, taking care to include the lumbar vertebra that is centered over the sacral spine in the lateral view.
 Thoracic screw placement is done after facetectomies at each corresponding level.
Thoracic screw placement is done after facetectomies at each corresponding level.Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 32: Patellar Instability: Lateral Release and Medial Plication
32: Patellar Instability: Lateral Release and Medial Plication
![]() 18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


56: Posterior Surgical Treatment for Scheuermann’s Kyphosis












