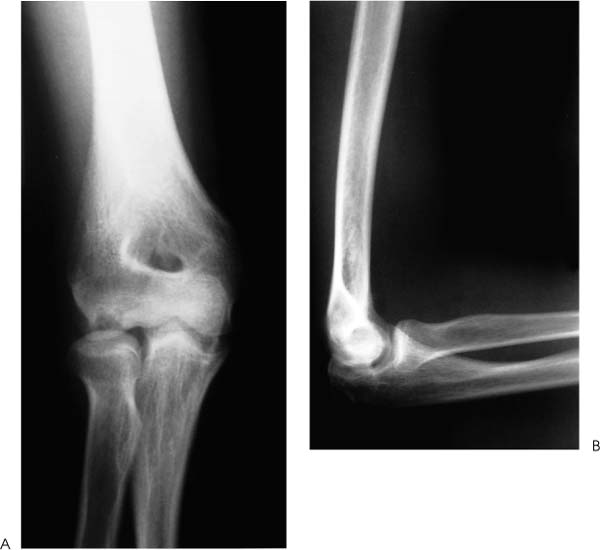
Case 56 A 15-year-old right-hand-dominant boy who is a baseball pitcher on his school team presents with a 3-month history of progressive lateral elbow pain and loss of motion. He also reports occasional swelling and locking symptoms. He states that occasionally he must manipulate the elbow to restore his motion. He denies any specific acute, traumatic event and reports symptoms have occurred insidiously. Range of motion of the elbow demonstrates an arc of 30 to 90 degrees of flexion. He has 60 degrees of supination and 60 degrees of pronation. There is a mild to moderate elbow effusion, with tenderness in the posterolateral gutter. Stability is grossly normal to valgus and varus examination. Figure 56–1. Anteroposterior (AP) (A) and lateral (B) radiographs of the elbow. 1. Rheumatologic illness 2. Osteochondritis dissecans 3. Medial ulnar collateral ligament disruption • Use of the soft spot portal is mandatory in confirming the extent of the osteochondritic lesion and is used in every case. PITFALL • Inability of the arthroscopist to adequately visualize the entire capitellum is an indication for open assessment of the capitellum. A low threshold for arthrotomy should be maintained so as to avoid underappreciating the extent of the osteochondritic lesion. Anteroposterior (AP) and lateral radiographs of the elbow are obtained (Fig. 56–1). Osteochondritis Dissecans. Limited range of motion and elbow effusion, a history of locking and catching in the elbow, and radiographic changes seen in the capitellum confirm the diagnosis of osteochondritis dissecans. Patientswho experience repetitive valgus stress of the elbow, as in baseball players or adolescent gymnasts, are at high risk of developing osteochondritis dissecans. These young patients usually present with an insidious onset of rather diffuse elbow pain and loss of motion. They sometimes relate a single traumatic episode, but often report no such event. Locking and catching symptoms are also not uncommon at presentation. Many patients complain of medial elbow symptoms including ulna neuritis and pain. These symptoms are presumably due to medial ulnar collateral ligament insufficiency from chronic overuse or traumatic disruption. All such patients with elbow pain should be examined for valgus instability of the elbow, with specific attention paid to the ulnar nerve.
History and Physical Examination
Differential Diagnosis
Radiologic Findings
Diagnosis
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


