• The anatomy of the hemilamina in relationship to the levels above and below must be understood to confirm being at the correct level.
Hemivertebra Resection
Examination/Imaging
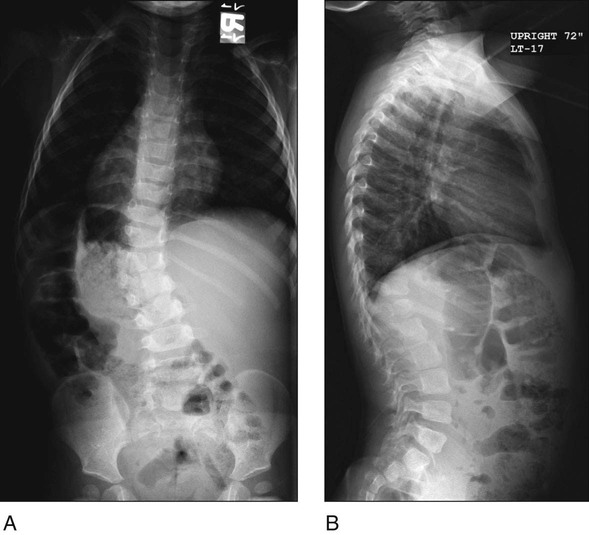
 Standing posteroanterior (PA) and lateral 36-inch spine radiographs are obtained. Figure 1 shows standing radiographs of a patient with a thoracolumbar hemivertebra in PA (Fig. 1A) and lateral (Fig. 1B) views.
Standing posteroanterior (PA) and lateral 36-inch spine radiographs are obtained. Figure 1 shows standing radiographs of a patient with a thoracolumbar hemivertebra in PA (Fig. 1A) and lateral (Fig. 1B) views.
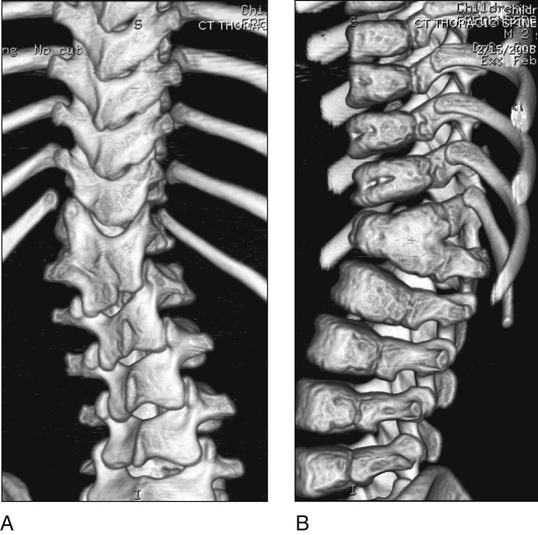
 Three-dimensional computed tomography (CT) scan will reveal the posterior elements (Fig. 2A) and the partial anterior fusion (Fig. 2B).
Three-dimensional computed tomography (CT) scan will reveal the posterior elements (Fig. 2A) and the partial anterior fusion (Fig. 2B).
 Screening examinations should be done for additional morbidities:
Screening examinations should be done for additional morbidities:
Surgical Anatomy
 The relevant surgical anatomy for hemivertebra excision relies on a thorough understanding of the posterior spinal elements as well as the anatomy of the hemivertebra posterior elements.
The relevant surgical anatomy for hemivertebra excision relies on a thorough understanding of the posterior spinal elements as well as the anatomy of the hemivertebra posterior elements.
 Understanding the anterior anatomy and whether or not the hemivertebra is segmented or partially segmented helps with complete resection anteriorly.
Understanding the anterior anatomy and whether or not the hemivertebra is segmented or partially segmented helps with complete resection anteriorly.
Positioning
 The patient is placed in the prone position on a radiolucent spinal frame.
The patient is placed in the prone position on a radiolucent spinal frame.
 Padding is placed on the chest and iliac crests, taking care to keep the abdomen free to facilitate venous return (Fig. 3).
Padding is placed on the chest and iliac crests, taking care to keep the abdomen free to facilitate venous return (Fig. 3).

 The patient must have appropriate somatosensory and motor evoked potential monitoring in place.
The patient must have appropriate somatosensory and motor evoked potential monitoring in place.
Portals/Exposures
 Standard posterior element exposure is done.
Standard posterior element exposure is done.
Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 32: Patellar Instability: Lateral Release and Medial Plication
32: Patellar Instability: Lateral Release and Medial Plication
![]() 18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


55: Hemivertebra Resection







