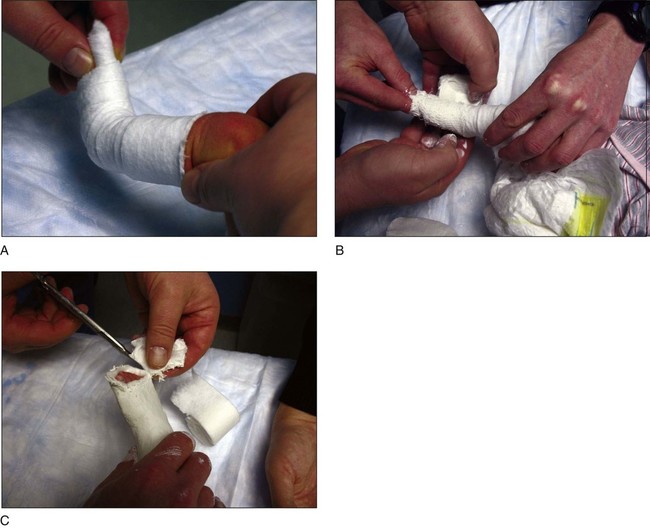
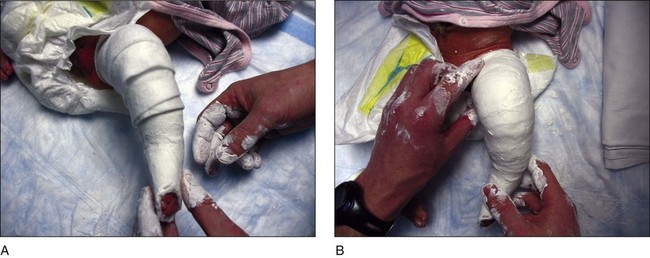
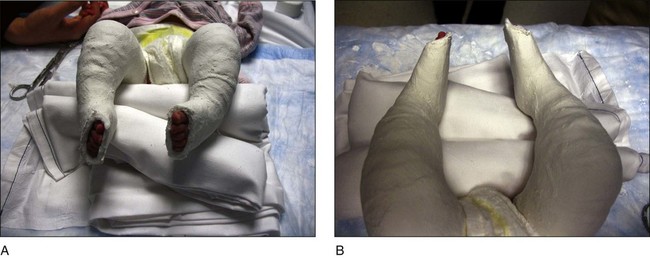
• The forefoot is placed in supination in line with the hindfoot, and the first ray is dorsiflexed. • Cast padding is applied to cover the toes distally (Fig. 3A). A plaster cast is applied using a 2-inch plaster roll (Fig. 3B). Cast should be cut distally so that all five toes are visible (Fig. 3C). • This will correct the cavus deformity. • A short-leg plaster cast is placed first, allowed to dry, and then extended up the thigh to create a long-leg cast. This technique is recommended for all subsequent casts. • Figure 6 shows the first cast for a patient with bilateral clubfoot deformity from below (Fig. 6A) and from above (Fig. 6B).
Ponseti Method for Idiopathic Clubfoot Deformity
Examination/Imaging
 Examination of the foot will demonstrate four components to the deformity:
Examination of the foot will demonstrate four components to the deformity:
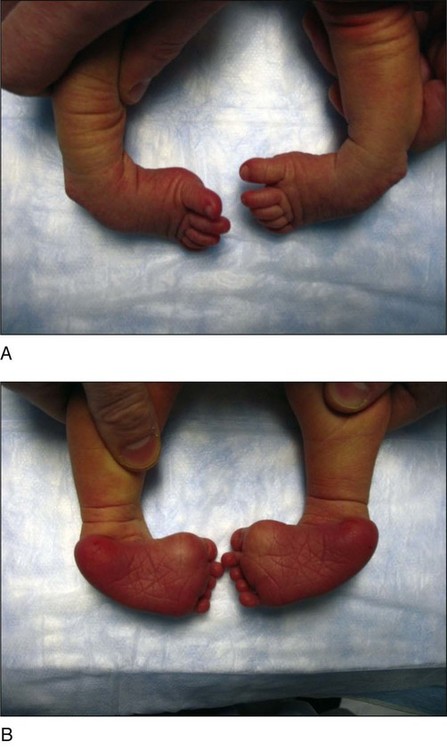
 Figure 1 shows a child with bilateral clubfoot deformity from the dorsal (Fig. 1A) and plantar (Fig. 1B) views.
Figure 1 shows a child with bilateral clubfoot deformity from the dorsal (Fig. 1A) and plantar (Fig. 1B) views.
 The flexibility of the deformity is assessed.
The flexibility of the deformity is assessed.
 Deep skin creases are often noted posteriorly and medially.
Deep skin creases are often noted posteriorly and medially.
 There is little role for imaging in the diagnosis of a clubfoot deformity.
There is little role for imaging in the diagnosis of a clubfoot deformity.
Procedure
Step 1
 Manipulations must always be gentle and never painful.
Manipulations must always be gentle and never painful.
 Approximately 1 minute is spent manipulating the foot.
Approximately 1 minute is spent manipulating the foot.
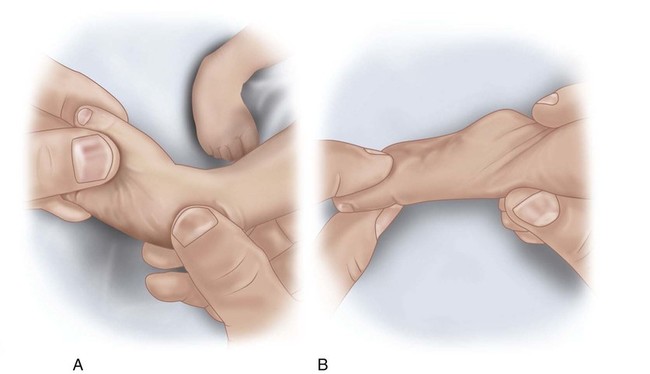
 Figure 2 demonstrates the first manipulation in an anteroposterior (AP) (Fig. 2A) and lateral (Fig. 2B) view. The forefoot is supinated in line with the hindfoot, and the first ray is dorsiflexed.
Figure 2 demonstrates the first manipulation in an anteroposterior (AP) (Fig. 2A) and lateral (Fig. 2B) view. The forefoot is supinated in line with the hindfoot, and the first ray is dorsiflexed.
 Correct positioning of the foot is maintained while the short-leg cast is allowed to dry (Fig. 4).
Correct positioning of the foot is maintained while the short-leg cast is allowed to dry (Fig. 4).

 One the short-leg plaster cast has hardened, the cast is extended up the thigh. Cast padding is applied first (Fig. 5A). Plaster is applied up to the proximal thigh (Fig. 5B).
One the short-leg plaster cast has hardened, the cast is extended up the thigh. Cast padding is applied first (Fig. 5A). Plaster is applied up to the proximal thigh (Fig. 5B).
Step 2
 With the cavus deformity corrected, the next few casts are placed so that the foot is gradually abducted around the head of the talus.
With the cavus deformity corrected, the next few casts are placed so that the foot is gradually abducted around the head of the talus.
 The foot is manipulated prior to placement of the second cast.
The foot is manipulated prior to placement of the second cast.
Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 32: Patellar Instability: Lateral Release and Medial Plication
32: Patellar Instability: Lateral Release and Medial Plication
![]() 1: Modified Woodward Procedure for Sprengel’s Deformity
1: Modified Woodward Procedure for Sprengel’s Deformity
 40: Proximal Tibial Osteotomy for Blount’s Disease
40: Proximal Tibial Osteotomy for Blount’s Disease
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


















