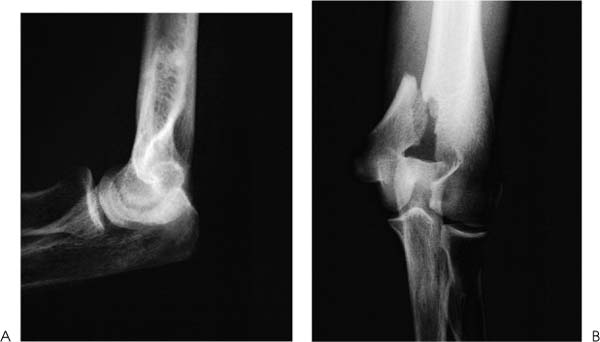
Case 31 A 21-year-old recreational soccer player presents 6 hours after falling onto an outstretched arm. He complains of pain, swelling, and limited motion of his elbow. He denies any numbness or weakness. Range of motion is 60 to 100 degrees of elbow flexion. He has moderate crepitation and pain through a range of motion and moderate swelling of his elbow. Stability testing demonstrates significant opening to valgus stress. He is neurovascularly intact. Figure 31–1. (A) Anteroposterior (AP) and (B) lateral radiographs demonstrate a medial condyle fracture. 1. Medial ulnar collateral ligament disruption 2. Intercondylar distal humerus fracture 3. Medial condyle fracture 4. Elbow dislocation Anteroposterior (AP) and lateral radiographs are obtained (Fig. 31–1). Medial Condyle Fracture. Pain, swelling, and crepitation point toward an elbow fracture. Increased valgus opening demonstrates the loss of bony or ligamentous integrity. Radiographs confirm a medial condyle fracture. The authors prefer open reduction and internal fixation of all but nondisplaced or minimally displaced medial condyle fractures. Generally, little comminution is present, allowing for good intraoperative and postoperative stability. The instability associated with the fracture itself and the disruption of the posterolateral ligamentous structures that often occurs argue against treating the fracture nonoperatively. The goal of surgery is to restore joint congruity with stable internal fixation, allowing for early postoperative motion. Generally, a medial incision is carried out and the ulnar nerve is carefully protected. Screw fixation is often adequate using lag screw AO techniques. A medial columnar plate should be placed if significant comminution is present or if lag screw fixation is deemed to provide inadequate stability to allow for immediate motion. Care must be taken to avoid the olecranon fossa with the screws, and intraoperative fluoroscopy is helpful in this regard. Also, AO cannulated screws are helpful in directing screw placement (Fig. 31–2). Repair of the lateral ulnar collateral ligament complex is considered if joint stability is not restored by fracture fixation. The varus stress usually responsible for medial condyle fractures results in disruption of this lateral ulnar collateral ligament complex. If, after fracture fixation, posterolateral rotatory subluxation persists, repair of the lateral capsular disruption should be accomplished through a separate, lateral incision. Suction drainage is usually applied and a soft dressing placed on the extremity. Figure 31–2. (A) AP and (B) lateral radiographs demonstrate fracture fixation. PEARLS • Adequate visualization at the time of fracture fixation is important in ensuring anatomic reduction. • Fluoroscopic evaluation of fracture alignment and fixation are important in helping confirm a good reduction and in ensuring that screws are properly positioned.
History and Physical Examination
Differential Diagnosis
Radiologic Findings
Diagnosis
Surgical Management

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


