Discoid Lateral Meniscus
Examination/Imaging
 Examination may show joint line tenderness, effusion, decreased range of motion, quadriceps atrophy, bulge at the anterolateral joint line in full flexion, click and shift of the meniscus on extension, and a positive McMurray’s sign.
Examination may show joint line tenderness, effusion, decreased range of motion, quadriceps atrophy, bulge at the anterolateral joint line in full flexion, click and shift of the meniscus on extension, and a positive McMurray’s sign.
 MRI should show continuity of the meniscus between the anterior and posterior horns on ≥ 3 consecutive sagittal sections that are 5 mm thick (Fig. 1).
MRI should show continuity of the meniscus between the anterior and posterior horns on ≥ 3 consecutive sagittal sections that are 5 mm thick (Fig. 1).

 MRI will help visualize tears and intrasubstance degeneration.
MRI will help visualize tears and intrasubstance degeneration.
Portals/Exposures
 Standard anterior medial and lateral portals are used (Fig. 3).
Standard anterior medial and lateral portals are used (Fig. 3).

 Midpatellar medial and lateral portals are added as required (see Fig. 3).
Midpatellar medial and lateral portals are added as required (see Fig. 3).
 A posterolateral incision is made as necessary for inside-out meniscal repairs.
A posterolateral incision is made as necessary for inside-out meniscal repairs.
 An anterolateral incision is made as necessary for outside-in meniscal repairs.
An anterolateral incision is made as necessary for outside-in meniscal repairs.
Procedure
Step 1: Arthroscopic Assessment
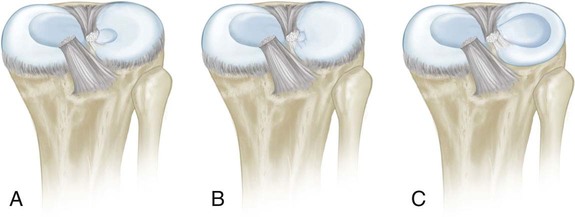
 The surgeon must visualize the discoid meniscus and determine its extent. Figure 4 shows an incomplete discoid meniscus.
The surgeon must visualize the discoid meniscus and determine its extent. Figure 4 shows an incomplete discoid meniscus.

 An assessment is made for tears and instability of the discoid meniscus.
An assessment is made for tears and instability of the discoid meniscus.
 The surgeon should assess for chondral damage, osteochondritis dissecans lesions, and loose bodies.
The surgeon should assess for chondral damage, osteochondritis dissecans lesions, and loose bodies.
Step 2: Partial Meniscectomy
Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 32: Patellar Instability: Lateral Release and Medial Plication
32: Patellar Instability: Lateral Release and Medial Plication
![]() 18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


31: Discoid Lateral Meniscus