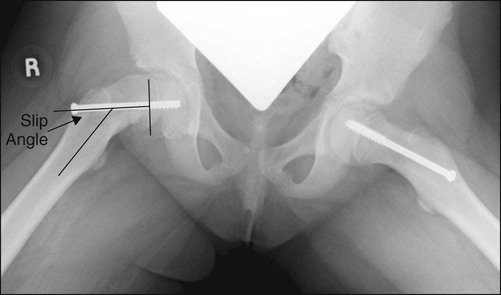
• The slip angle is the angle between a line perpendicular to the epiphysis and a line parallel to the femoral shaft on the lateral radiograph (see Fig. 2). • The deep branch of the medial femoral circumflex artery constitutes the main blood supply to the femoral head (see Fig. 5). This artery lies anterior to the obturator externus tendon and may be damaged by vigorous retraction in this area. • The trochanteric branch is visible on the lateral-posterior aspect of the trochanter during the surgical approach. The trochanteric branch is at the level of the obturator externus tendon and therefore serves as a rough landmark for the medial femoral circumflex artery.
Flexion Osteotomy for Slipped Capital Femoral Epiphysis
Examination/Imaging
 The hip is examined for range of motion. It is especially important to document deficiency of internal rotation and flexion as these may be corrected with rotation and flexion through the osteotomy. Extension, abduction, and adduction should also be recorded.
The hip is examined for range of motion. It is especially important to document deficiency of internal rotation and flexion as these may be corrected with rotation and flexion through the osteotomy. Extension, abduction, and adduction should also be recorded.
 Any leg length discrepancy should be noted as this may be corrected with the osteotomy.
Any leg length discrepancy should be noted as this may be corrected with the osteotomy.
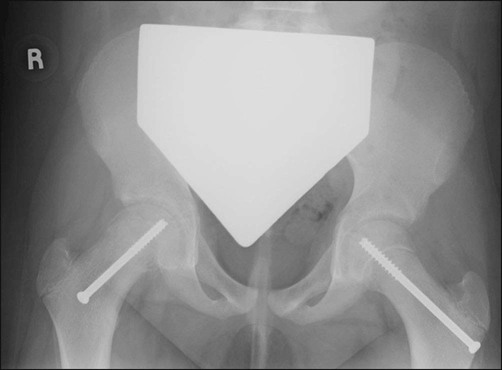
 Anteroposterior (AP) (Fig. 1) and lateral (Fig. 2) radiographs of the affected hip must be obtained. The slip angle should be determined from the lateral radiograph.
Anteroposterior (AP) (Fig. 1) and lateral (Fig. 2) radiographs of the affected hip must be obtained. The slip angle should be determined from the lateral radiograph.
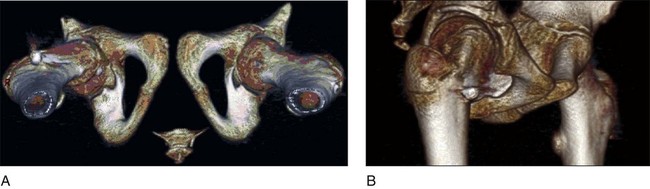
 A computed tomography (CT) scan of the proximal femur with three-dimensional rendering may provide the surgeon with a better understanding of the deformity (Fig. 3A and 3B).
A computed tomography (CT) scan of the proximal femur with three-dimensional rendering may provide the surgeon with a better understanding of the deformity (Fig. 3A and 3B).
Surgical Anatomy
 Superficial anatomy includes the gluteus maximus muscle, tensor fascia lata muscle, and iliotibial band (Fig. 4).
Superficial anatomy includes the gluteus maximus muscle, tensor fascia lata muscle, and iliotibial band (Fig. 4).
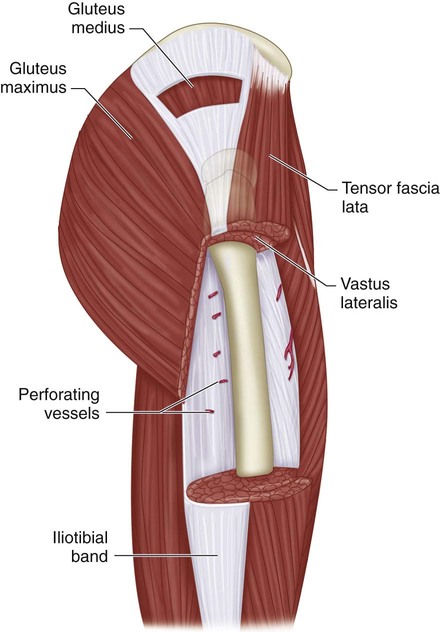
 Deep anatomy includes the gluteus medius and vastus lateralis muscles.
Deep anatomy includes the gluteus medius and vastus lateralis muscles.
 Perforating vessels may be found entering the vastus lateralis through the intermuscular septum (see Fig. 4). These vessels should be identified and coagulated as the vastus lateralis is reflected off the intermuscular septum and lateral aspect of the femur.
Perforating vessels may be found entering the vastus lateralis through the intermuscular septum (see Fig. 4). These vessels should be identified and coagulated as the vastus lateralis is reflected off the intermuscular septum and lateral aspect of the femur.
 The vastus ridge is the site of insertion of both the gluteus medius and vastus lateralis muscles (Fig. 5). This bony landmark is useful for planning the osteotomy.
The vastus ridge is the site of insertion of both the gluteus medius and vastus lateralis muscles (Fig. 5). This bony landmark is useful for planning the osteotomy.

 It is important to understand the blood supply to the femoral head.
It is important to understand the blood supply to the femoral head.
Positioning
Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 32: Patellar Instability: Lateral Release and Medial Plication
32: Patellar Instability: Lateral Release and Medial Plication
![]() 18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Musculoskeletal Key
Fastest Musculoskeletal Insight Engine




