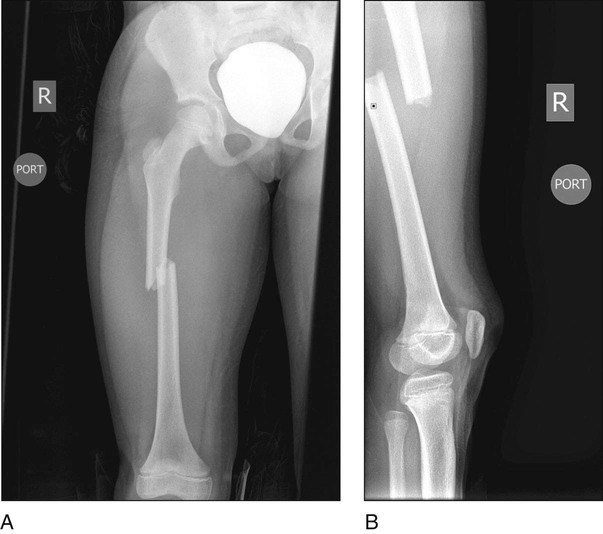
• Note the mechanism of injury. • Examine the skin, surrounding soft tissue, and neurovascular status. In isolated femur fracture, the thigh is swollen and bruised. • Examine other organs and injuries in cases of high-energy trauma. • Figure 1 shows AP (Fig. 1A) and lateral (Fig. 1B) radiographs of a mid-diaphyseal femur fracture. • Radiographs should include one joint above and below the fracture. • The affected leg is abducted 15–30°, allowing working on both sides of the femur (Fig. 3). • The white arrow between the legs in Figure 3 depicts the position of the image intensifier.
Femur Fracture
Flexible Intramedullary Nailing
Examination/Imaging
 A thorough physical examination is conducted.
A thorough physical examination is conducted.
Surgical Anatomy
 The distal femoral physis is marked under fluoroscopy to avoid any inadvertent injury to the physis.
The distal femoral physis is marked under fluoroscopy to avoid any inadvertent injury to the physis.
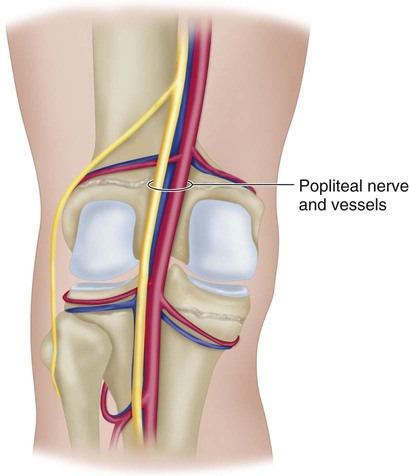
 The popliteal vessels and the nerve are posterior to the femur at the surgical site (Fig. 2). Avoid slippage of the drill posteriorly while drilling the lateral and medial holes.
The popliteal vessels and the nerve are posterior to the femur at the surgical site (Fig. 2). Avoid slippage of the drill posteriorly while drilling the lateral and medial holes.
Positioning
 The patient is positioned supine on a radiolucent table or a fracture table (our preference).
The patient is positioned supine on a radiolucent table or a fracture table (our preference).

Procedure
Step 1
 After adequate positioning of the patient on a fracture table, the fracture is reduced as best as possible. The leg is prepared and draped in a standard manner either on the fracture table or on a radiolucent table.
After adequate positioning of the patient on a fracture table, the fracture is reduced as best as possible. The leg is prepared and draped in a standard manner either on the fracture table or on a radiolucent table.
 The distal femoral physis is identified under an image intensifier (Fig. 4), and the nail entry sites are marked 2 cm proximal to the physis on the medial and lateral distal femoral metaphyses.
The distal femoral physis is identified under an image intensifier (Fig. 4), and the nail entry sites are marked 2 cm proximal to the physis on the medial and lateral distal femoral metaphyses.Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 32: Patellar Instability: Lateral Release and Medial Plication
32: Patellar Instability: Lateral Release and Medial Plication
![]() 1: Modified Woodward Procedure for Sprengel’s Deformity
1: Modified Woodward Procedure for Sprengel’s Deformity
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


21: Femur Fracture: Flexible Intramedullary Nailing











