• Gait is variably antalgic with a universal external foot progression angle component. • Passive hip range of motion reveals a decrease in flexion and internal rotation, with variable reduction in abduction. • In moderate and severe SCFE, terminal flexion is coupled with obligate external rotation (as a result of anterior neck impingement). Pearls • Prior to prepping the patient, check with fluoroscopy to ensure that the appropriate orthogonal images can be obtained.
Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis
Examination/Imaging
 Symptoms and physical findings vary according to the stability of the physis, chronicity of presentation, and severity of the slip.
Symptoms and physical findings vary according to the stability of the physis, chronicity of presentation, and severity of the slip.
 Patients with stable SCFE exhibit a spectrum of clinical findings.
Patients with stable SCFE exhibit a spectrum of clinical findings.
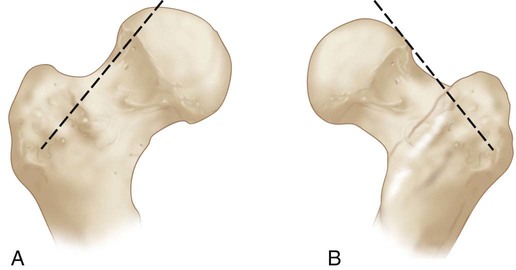
 Both anteroposterior (AP) and lateral radiographs are essential for diagnosis. Slips first displace posteriorly, where the AP radiographic findings may be subtle. A line drawn tangential to the superior femoral neck on the AP radiograph (Klein’s line) will intersect a smaller portion of the capital epiphysis (Fig. 1A) or not intersect at all (Trethowan’s sign; Fig. 1B) compared to the uninvolved hip.
Both anteroposterior (AP) and lateral radiographs are essential for diagnosis. Slips first displace posteriorly, where the AP radiographic findings may be subtle. A line drawn tangential to the superior femoral neck on the AP radiograph (Klein’s line) will intersect a smaller portion of the capital epiphysis (Fig. 1A) or not intersect at all (Trethowan’s sign; Fig. 1B) compared to the uninvolved hip.
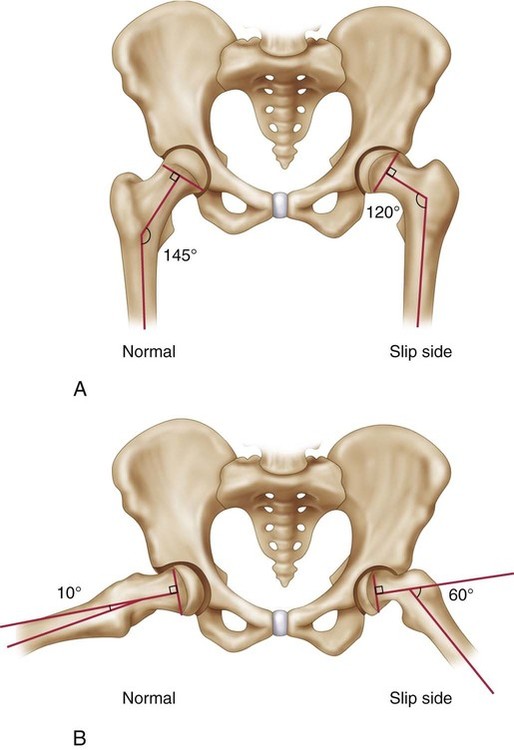
 Southwick classified the degree of slippage by measuring the femoral head-shaft angle on the AP (Fig. 2A) or frog-leg lateral (Fig. 2B) view.
Southwick classified the degree of slippage by measuring the femoral head-shaft angle on the AP (Fig. 2A) or frog-leg lateral (Fig. 2B) view.
 Radiographic examination of the contralateral hip in AP (Fig. 3) and frog-leg lateral (Fig. 4) views at the time of surgery is critical as the incidence of bilateral involvement at initial presentation is at least 25%.
Radiographic examination of the contralateral hip in AP (Fig. 3) and frog-leg lateral (Fig. 4) views at the time of surgery is critical as the incidence of bilateral involvement at initial presentation is at least 25%.


Positioning
 The position of choice is supine on a radiolucent operating table.
The position of choice is supine on a radiolucent operating table.
 Great care must be taken to position the patient with an unstable slip.
Great care must be taken to position the patient with an unstable slip.
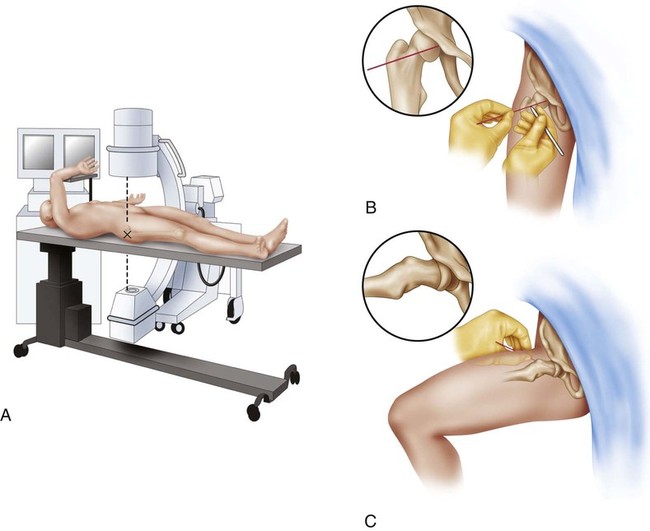
 Once on the fracture table, position the ipsilateral arm across the body to give the C-arm the greatest space for operation (Fig. 6A–C).
Once on the fracture table, position the ipsilateral arm across the body to give the C-arm the greatest space for operation (Fig. 6A–C).
Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 32: Patellar Instability: Lateral Release and Medial Plication
32: Patellar Instability: Lateral Release and Medial Plication
![]() 1: Modified Woodward Procedure for Sprengel’s Deformity
1: Modified Woodward Procedure for Sprengel’s Deformity
![]() 47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
47: Resection of Calcaneonavicular Coalition and Fat Autograft Interposition
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


18: Percutaneous in situ Cannulated Screw Fixation of Slipped Capital Femoral Epiphysis