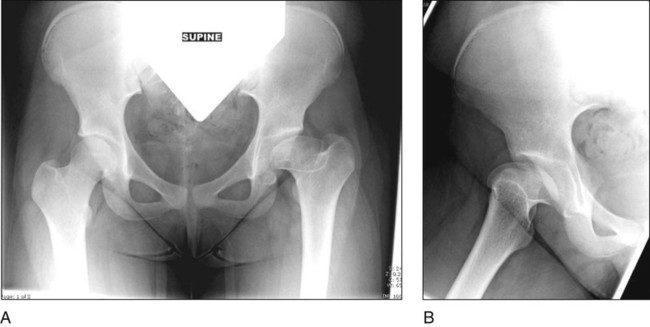
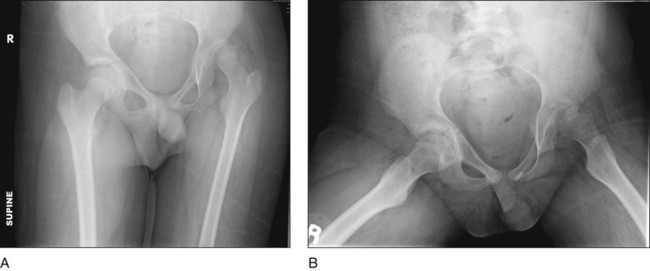
• Figure 1 shows preoperative anteroposterior (AP) (Fig. 1A) and lateral (Fig. 1B) radiographs of a patient with right hip Legg-Calvé-Perthes disease. • Figure 2 shows preoperative AP (Fig. 2A) and frog lateral (Fig. 2B) radiographs of a candidate for Chiari pelvic osteotomy. • The Von Rosen view can demonstrate the incongruous relationship between the femoral head and acetabulum and also demonstrate the reducibility of the femoral head within the acetabulum.
Chiari Pelvic Osteotomy
Examination/Imaging
Physical Examination
 Examination should begin with observed gait analysis to document if a limp is present and if it is a result of antalgia or Trendelenburg dysfunction.
Examination should begin with observed gait analysis to document if a limp is present and if it is a result of antalgia or Trendelenburg dysfunction.
 The Galleazzi sign is significant for fixed hip instability and subluxation/dislocation.
The Galleazzi sign is significant for fixed hip instability and subluxation/dislocation.
Imaging Studies
 Imaging studies are designed to document the congruency of the femoral head within the acetabulum, the amount of anterior and lateral acetabular coverage of the femoral head, and the reducibility of the femoral head into the native acetabulum.
Imaging studies are designed to document the congruency of the femoral head within the acetabulum, the amount of anterior and lateral acetabular coverage of the femoral head, and the reducibility of the femoral head into the native acetabulum.
 Reconstructed computed tomography scans can aid surgeons in determining the three-dimensional relationship between the acetabulum and femoral head and identifying locations of acetabular deficiency (anterolateral vs. posterolateral).
Reconstructed computed tomography scans can aid surgeons in determining the three-dimensional relationship between the acetabulum and femoral head and identifying locations of acetabular deficiency (anterolateral vs. posterolateral).
Surgical Anatomy
 In the ilioinguinal approach to the hip, superficially the lateral femoral cutaneous nerve (LFCN) is at risk in the interval between the sartorius muscle medially and the tensor fascia lata (TFL) muscle laterally. By remaining in the compartment of the TFL, the LFCN is protected during the surgical approach.
In the ilioinguinal approach to the hip, superficially the lateral femoral cutaneous nerve (LFCN) is at risk in the interval between the sartorius muscle medially and the tensor fascia lata (TFL) muscle laterally. By remaining in the compartment of the TFL, the LFCN is protected during the surgical approach.
Positioning
 The patient is positioned supine on a radiolucent operating room table.
The patient is positioned supine on a radiolucent operating room table.
 Often a bump is placed under the operative hip to achieve a “sloppy lateral” position.
Often a bump is placed under the operative hip to achieve a “sloppy lateral” position.
 All bony prominences on the upper and lower extremities are padded.
All bony prominences on the upper and lower extremities are padded.
 The operative extremity is draped free to the level of the costophrenic margin superiorly, medially to the ipsilateral border of the perineum, and laterally to the border of the buttocks. Figure 3 shows skin markings for a planned ilioinguinal approach and a direct lateral approach to the proximal femur for an additional intertrochanteric osteotomy.
The operative extremity is draped free to the level of the costophrenic margin superiorly, medially to the ipsilateral border of the perineum, and laterally to the border of the buttocks. Figure 3 shows skin markings for a planned ilioinguinal approach and a direct lateral approach to the proximal femur for an additional intertrochanteric osteotomy.

 Intraoperative fluoroscopy is employed from the contralateral side of the bed.
Intraoperative fluoroscopy is employed from the contralateral side of the bed.
Portals/Exposures
 The ilioinguinal approach is the exposure of choice for this osteotomy. In Figure 4, the iliac crest is marked with the direct head of the rectus femoris (arrow) deep to the TFL compartment (TFL retracted posteriorly).
The ilioinguinal approach is the exposure of choice for this osteotomy. In Figure 4, the iliac crest is marked with the direct head of the rectus femoris (arrow) deep to the TFL compartment (TFL retracted posteriorly).Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 32: Patellar Instability: Lateral Release and Medial Plication
32: Patellar Instability: Lateral Release and Medial Plication
![]() 1: Modified Woodward Procedure for Sprengel’s Deformity
1: Modified Woodward Procedure for Sprengel’s Deformity
 40: Proximal Tibial Osteotomy for Blount’s Disease
40: Proximal Tibial Osteotomy for Blount’s Disease
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


12: Chiari Pelvic Osteotomy

















