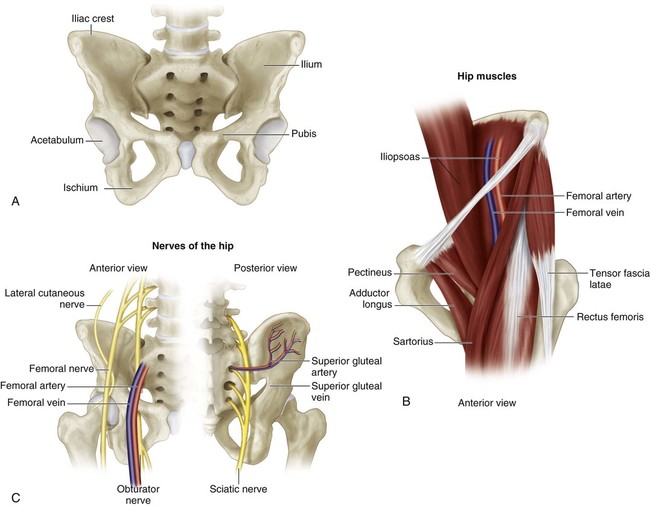
• Bones (Fig. 2A): iliac apophysis, iliac crest, greater sciatic notch, acetabular labrum and lateral acetabular epiphysis • Muscles and ligamentous complexes (Fig. 2B): sartorius and tensor fascia femoris, straight head of the rectus femoris, transverse acetabular ligament, ligamentum teres, iliopsoas muscle/tendon • Nerves (Fig. 2C): lateral femoral cutaneous nerve of the thigh, superior gluteal nerve • Vessels in the greater sciatic notch and the surrounding soft tissues of the ilium (see Fig. 2C) • Just distal to this point, the tendon is tagged with a suture for later repair and then transected. The reflected head is separated from the capsule and detached from the ilium posteriorly to just beyond the most proximal point of the dislocated femoral head. • If the hip is not dislocated, the rectus femoris may be left intact as the innominate osteotomy is done just proximal to the insertion of the straight head into the anterior inferior iliac spine. Pearls
Innominate Osteotomy
Surgical Anatomy
 The surgeon should be familiar with the following anatomic structures:
The surgeon should be familiar with the following anatomic structures:
Portals/Exposures
 A transverse “bikini line” incision is made centered on and just distal to the anterior superior iliac spine.
A transverse “bikini line” incision is made centered on and just distal to the anterior superior iliac spine.
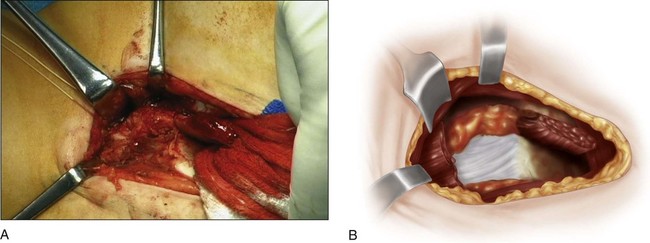
 The iliac crest is stripped subperiosteally both medially and laterally to the greater sciatic notch (Fig. 4A and 4B). Rang sciatic notch retractors (Fig. 5) facilitate protection of the superior gluteal nerve and vessels in the notch and the surrounding soft tissues when cutting the ilium with the Gigli saw.
The iliac crest is stripped subperiosteally both medially and laterally to the greater sciatic notch (Fig. 4A and 4B). Rang sciatic notch retractors (Fig. 5) facilitate protection of the superior gluteal nerve and vessels in the notch and the surrounding soft tissues when cutting the ilium with the Gigli saw.

Procedure
Step 1
 Prior to making the skin incision, a percutaneous tenotomy of the adductor longus is done.
Prior to making the skin incision, a percutaneous tenotomy of the adductor longus is done.
 An anterolateral approach via a transverse (bikini line) incision is used (see Portals/Exposures).
An anterolateral approach via a transverse (bikini line) incision is used (see Portals/Exposures).
 If the innominate osteotomy is being done for dysplasia or mild subluxation, proceed to Step 7.
If the innominate osteotomy is being done for dysplasia or mild subluxation, proceed to Step 7.
Step 2 (When Hip Is Dislocated)
 The capsule is cleared anteromedially of soft tissue, including the overlying iliopsoas, with a periosteal elevator.
The capsule is cleared anteromedially of soft tissue, including the overlying iliopsoas, with a periosteal elevator.
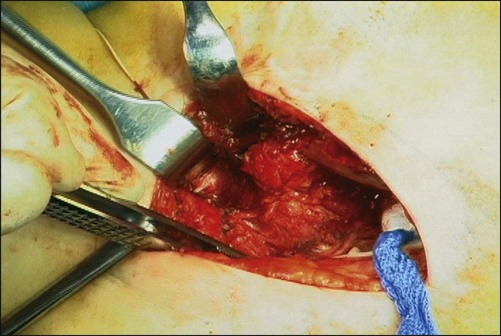
 The capsule is now exposed from the level of the transverse acetabular ligament to the top of the femoral head (Fig. 6).
The capsule is now exposed from the level of the transverse acetabular ligament to the top of the femoral head (Fig. 6).
Related posts:
![]() 41: Operative Treatment of Tillaux Fractures of the Ankle
41: Operative Treatment of Tillaux Fractures of the Ankle
 7: Forearm Fractures: Closed Treatment
7: Forearm Fractures: Closed Treatment
![]() 32: Patellar Instability: Lateral Release and Medial Plication
32: Patellar Instability: Lateral Release and Medial Plication
![]() 1: Modified Woodward Procedure for Sprengel’s Deformity
1: Modified Woodward Procedure for Sprengel’s Deformity
 40: Proximal Tibial Osteotomy for Blount’s Disease
40: Proximal Tibial Osteotomy for Blount’s Disease
 60: Thoracoscopic Release and Instrumentation for Scoliosis
60: Thoracoscopic Release and Instrumentation for Scoliosis
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


11: Innominate Osteotomy