Chapter 78 Hand Infections
General Approach to Hand Infections
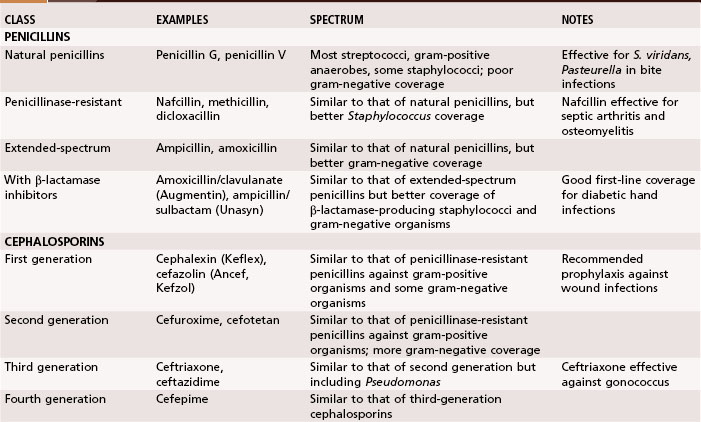
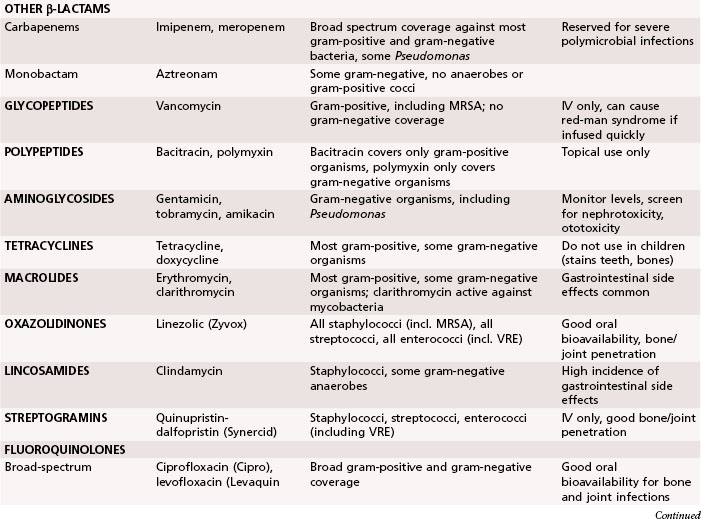
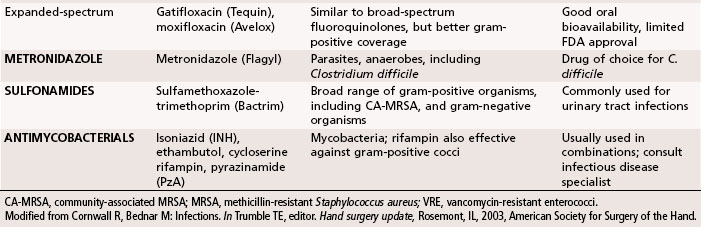
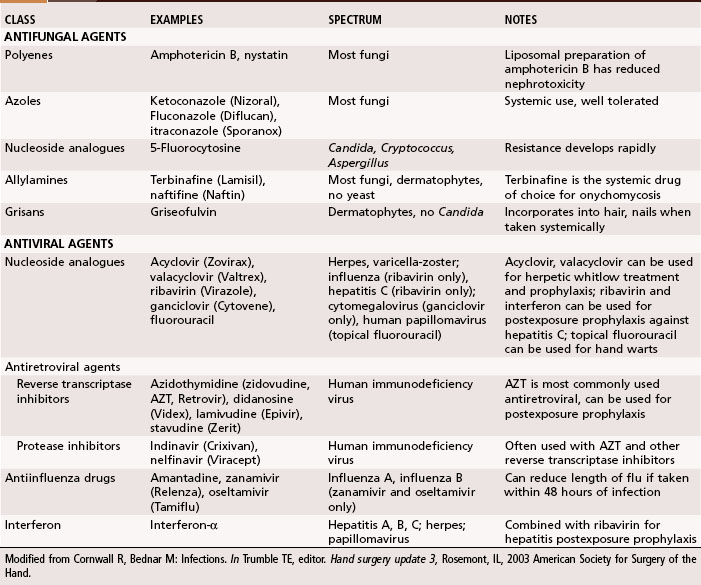
Antibiotics traditionally recommended for hand infections include a penicillinase-resistant penicillin or cephalosporin. When selecting antibiotics, it is important to be aware of the prevalence of antibiotic-resistant bacteria, such as methicillin-resistant S. aureus (MRSA), which is growing in prevalence in hand infections. Antibiotic resistance is seen in up to 65% of Staphylococcus cultures. Vancomycin is effective against the gram-positive organisms, whereas ciprofloxacin is most effective against the gram-negative organisms. The addition of antibiotics effective against gram-negative organisms has been recommended for high-risk situations, such as infections in intravenous drug users and contaminated outdoor or farm injuries. In Tables 78-1 and 78-2 a summary is provided of the appropriate use of antibiotics, antifungal agents, and antiviral agents. Because of the constantly changing inventory of antibiotics and the variations in patient populations and wound flora, antibiotic selection should be based on a variety of considerations and include the assistance of an infectious disease specialist when needed.





Paronychia
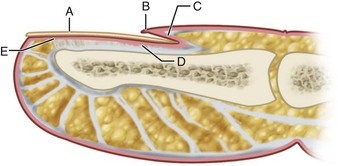
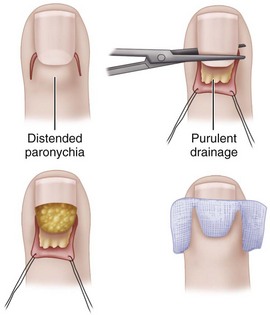
A paronychia (“runaround”) infection usually is caused by the introduction of S. aureus into the soft tissue fold around the fingernail (eponychium) associated with a hangnail or poor nail hygiene (Fig. 78-1). When an abscess forms in the eponychial or paronychial fold, it is known as a paronychia. It usually begins at one corner of the horny nail and travels under either the eponychium or the nail toward the opposite side. If an abscess is on one side only, it should be incised, angling the knife away from the nail to avoid cutting the nail bed, which would cause a ridge later. If the abscess is under one corner of the nail root, this corner should be removed. If it has already migrated to the opposite side and under the nail, a second incision should be made there, the skin folded back proximally, and the proximal one third of the nail excised. The wound is loosely packed with iodoform gauze for 48 hours for drainage (Fig. 78-2).
Chronic Paronychia
Eponychial Marsupialization
(BEDNAR AND LANE; KEYSER AND EATON)
 After administering a digital block anesthetic, cleanse the finger with antiseptic and drape it appropriately.
After administering a digital block anesthetic, cleanse the finger with antiseptic and drape it appropriately.
 Excise a crescent of skin 3 mm wide parallel to the eponychium and extending from the radial to the ulnar borders (Fig. 78-3).
Excise a crescent of skin 3 mm wide parallel to the eponychium and extending from the radial to the ulnar borders (Fig. 78-3).

 If nail irregularities are present, remove the nail.
If nail irregularities are present, remove the nail.

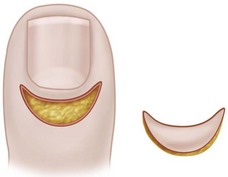
FIGURE 78-3 Eponychial marsupialization for treatment of paronychia. Symmetrical, crescent-shaped segment of skin is excised from dorsum of distal phalanx, leaving adequate bridge of skin and cuticle. SEE TECHNIQUE 78-2.
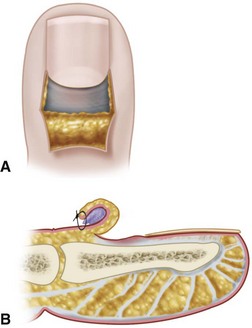
Pabari et al. described a “Swiss roll” technique for treatment of both acute and chronic paronychia in which the nail fold is elevated and reflected proximally over a nonadherent dressing and secured to the skin with a nonabsorbable suture (Fig. 78-4). Cited advantages of this technique are retention of the nail plate, rapid healing, and avoidance of a skin defect in the finger.
Felon
Incision and Drainage of Felons
 When the abscess points volarward, causing necrosis of the overlying skin, drain it by excising the necrotic skin.
When the abscess points volarward, causing necrosis of the overlying skin, drain it by excising the necrotic skin.
 When the abscess is in the distal pulp area pointing volarward toward the whorl of the fingerprint, it is best drained by a vertical incision begun distal to the skin crease and placed precisely in the midline to avoid the lateral branches of the digital nerve and to allow healing with minimal scar (Fig. 78-5).
When the abscess is in the distal pulp area pointing volarward toward the whorl of the fingerprint, it is best drained by a vertical incision begun distal to the skin crease and placed precisely in the midline to avoid the lateral branches of the digital nerve and to allow healing with minimal scar (Fig. 78-5).
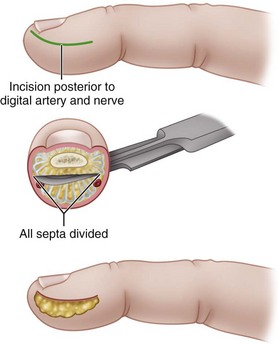
 If the abscess is deep and is partitioned by the septa, make a longitudinal incision, usually away from the contact area of the finger, cutting through the partitions (Fig. 78-6).
If the abscess is deep and is partitioned by the septa, make a longitudinal incision, usually away from the contact area of the finger, cutting through the partitions (Fig. 78-6).

 Irrigate the wound copiously, and pack it with iodoform gauze or sterile gauze bandage.
Irrigate the wound copiously, and pack it with iodoform gauze or sterile gauze bandage.

FIGURE 78-5 Midline vertical incision for drainage of abscess pointing volarward in distal pulp of finger. SEE TECHNIQUE 78-3.
Subfascial Space Infections
The potential spaces in the subfascial and deeper layers of the hand are infrequently infected. A high level of suspicion should lead to their detection and treatment. The recognized deep spaces of the hand include the interdigital web spaces, the midpalmar space, the thenar space, a less well-defined hypothenar space, the Parona space, and the dorsal subaponeurotic space (Fig. 78-7).
Web Space Infection (Collar Button Abscess)
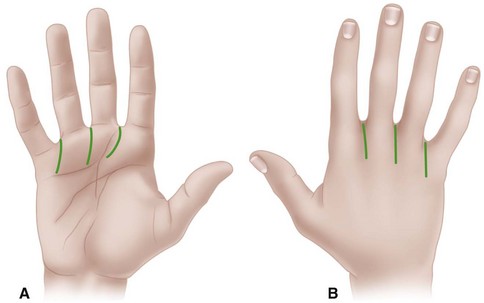
Web space infection usually localizes in one of the three fat-filled interdigital spaces just proximal to the superficial transverse ligament at the level of the metacarpophalangeal joints. Typically, the infection begins beneath palmar calluses in laborers. It may begin near the palmar surface, but because the skin and fascia here are less yielding, it may localize to drain dorsally. Here the tissue becomes obviously swollen, but the significant amount of the abscess remains nearer the palm. This may be the more dangerous part because, unless drained, it may spread through the lumbrical canal into the middle palmar space. Two longitudinal incisions usually are necessary for drainage: one on the dorsal surface between the metacarpal heads and the other on the palm, beginning distal to the distal palmar crease and curving proximally. Crossing the palmar creases at right angles to the crease should be avoided (Fig. 78-8). The web should not be incised.
Deep Fascial Space Infections
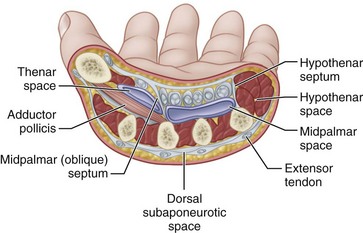
The palmar fascial space lies between the fascia covering the metacarpals and their contiguous muscles and the fascia dorsal to the flexor tendons. Its ulnar border is the fascia of the hypothenar muscles, and its radial border is the fascia of the adductor and other thenar muscles. This space is divided into a middle palmar space and a thenar space by a fascial membrane that passes obliquely from the third metacarpal shaft to the fascia dorsal to the flexor tendons of the index finger (Fig. 78-9). The hypothenar space has as its boundaries: the hypothenar septum laterally, the fifth metacarpal dorsally, and the hypothenar muscle fascia medially and palmar. The space of Parona is bordered by the pronator quadratus dorsally, the flexor pollicis longus laterally, the flexor carpi ulnaris medially, and the flexor tendons on the palmar aspect; it rarely is the site of abscess formation. Infections in these spaces are now rare because less extensive infections nearby usually are controlled by antibiotics before they spread. Abscesses in these spaces usually result from the spread of infection from other parts of the hand, typically from purulent flexor tenosynovial infections.
Incision and Drainage of Deep Fascial Space Infection
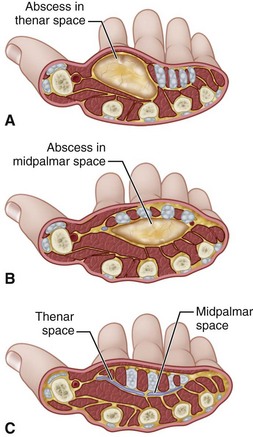
 Drain the middle palmar space through a curved incision beginning at the level of the distal palmar crease, in line with the long finger and extending ulnarward to just inside the hypothenar eminence (Fig. 78-10). Other options include the longitudinal distal palm incision and the transverse palm incision.
Drain the middle palmar space through a curved incision beginning at the level of the distal palmar crease, in line with the long finger and extending ulnarward to just inside the hypothenar eminence (Fig. 78-10). Other options include the longitudinal distal palm incision and the transverse palm incision.

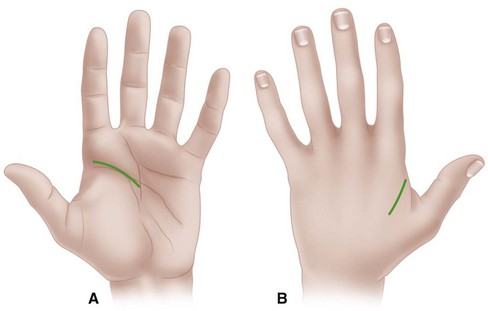
 Drain the thenar space through a curved incision in the thumb web parallel to the border of the first dorsal interosseous muscle or along the medial side of the thenar crease (Fig. 78-11). Avoid the recurrent branch of the median nerve at the proximal end of this crease. Avoid sharp, deep dissection, using blunt dissection to delineate the extent of the abscess.
Drain the thenar space through a curved incision in the thumb web parallel to the border of the first dorsal interosseous muscle or along the medial side of the thenar crease (Fig. 78-11). Avoid the recurrent branch of the median nerve at the proximal end of this crease. Avoid sharp, deep dissection, using blunt dissection to delineate the extent of the abscess.

 Retract the flexor tendons and median nerve, protecting them.
Retract the flexor tendons and median nerve, protecting them.




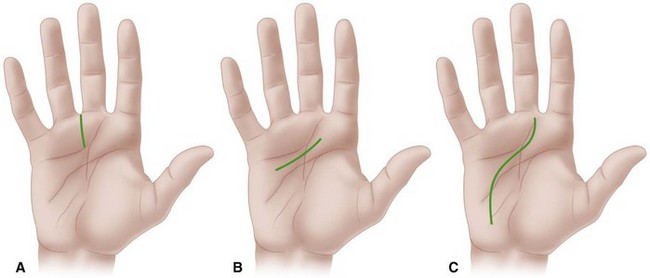
FIGURE 78-10 A, Distal longitudinal palmar incision. B, Transverse palmar incision. C, Extended longitudinal palmar incision. SEE TECHNIQUE 78-4.
Tenosynovitis
Postoperative Closed Irrigation
 With the patient under suitable anesthesia and after appropriately preparing and draping the hand and arm, inflate a pneumatic tourniquet; however, to reduce the risk of spreading the infection, do not wrap the limb.
With the patient under suitable anesthesia and after appropriately preparing and draping the hand and arm, inflate a pneumatic tourniquet; however, to reduce the risk of spreading the infection, do not wrap the limb.
 Expose the proximal end of the flexor sheath in the region of the A1 pulley by a straight transverse incision parallel to the distal palmar crease or by a zigzag incision in this area (Fig. 78-12). Expect to see serosanguineous or purulent fluid in the sheath.
Expose the proximal end of the flexor sheath in the region of the A1 pulley by a straight transverse incision parallel to the distal palmar crease or by a zigzag incision in this area (Fig. 78-12). Expect to see serosanguineous or purulent fluid in the sheath.
 Open the sheath proximal to the A1 pulley, and swab the fluid to send for cultures.
Open the sheath proximal to the A1 pulley, and swab the fluid to send for cultures.

 As an alternative, carefully make a transverse incision over the distal flexion crease.
As an alternative, carefully make a transverse incision over the distal flexion crease.
 Open the flexor sheath distal to the A4 pulley.
Open the flexor sheath distal to the A4 pulley.


Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


