Fig. 21.1
Wave jumping. In this discipline, the peaks of unbroken waves are used like a ramp allowing athletes to perform aerial stunts. Wave sailing is the most extreme discipline in windsurfing, which is practiced in strong wind conditions and large waves (Photo: Claudio Marosa)
21.1.3 Equipment
The equipment used in windsurfing varies considerably depending on a number of factors including weather conditions and the particular discipline practiced. In Formula Windsurfing, the highest performance course racing class, equipment is used with the largest surface area since events involve sailing upwind and are even held in light winds. Sail sizes can reach 12.5 m2 and boards may have widths of up to 1 m with fins measuring up to 70 cm in length. Wave boards, at the other extreme, are small, light and highly maneuverable: the volume in liters is generally comparable to the weight of the sailor in kilograms, while the sail area is commonly in the range of 4–6 m2.
In slalom events, equipment is designed to achieve top speed because there are no path distances upwind, and a minimum wind speed of 11 knots (20 km/h) is required for races [11]. Freestyle equipment is similar to wave equipment but considerably larger and specifically shaped to perform acrobatic tricks on flat water, including jumps, rotations, slides, flips and loops. The discipline known as free riding is a recreational style in which athletes use various sizes of boards dependent on weather conditions and their own preferences. Fairly large boards (around 130 l) and well-controllable sails (approximately 6–7 m2) are preferred [12]. Speed events involve the use of special, extremely narrow boards launched at speeds of over 45 knots on flat water with the aim of setting new speed records.
21.1.4 Sailing Technique
Windsurfers can sail both in displacement mode, cutting through the water like a sailboat, or preferably in planing mode, skipping over the water’s surface when the wind speed exceeds 10 knots (about 19 km/h). When planing, the windsurfers maintain the sail rig in a back position on the board, their feet are in the foot straps, and they are typically attached to the mast by means of a harness to counterbalance wind pressure on the sail. As wind strength increases, equipment decreases in size; boards with lower volumes and shorter in length and width and sails with a reduced surface area are preferred. The directional control of the windsurf is mainly achieved by the rider shifting his/her weight and adjusting the position of the rig with respect to the board. As in sailing, the main windsurfing maneuvers are tack and jibe with the exception of wave riding where heel side turns while planing (cutbacks) are the only maneuvers used (Fig. 21.2

).
Fig. 21.2
In wave riding, the windsurfer rides the face of a wave performing narrow-linked turns such as bottom turns, cutbacks and top turns (Photo: Claudio Marosa)
21.2 Injuries and Illnesses
Although windsurfing enjoys the reputation of being a fairly safe activity, a number of injuries may occur including acute and overuse injuries. When practicing windsurfing, the management of common injuries such as wounds requires specific precautions. Infectious diseases are also reported and occur due to the fact that windsurfing is often tolerated in areas where bathing is not considered to be safe because of water pollution.
21.3 Acute Injuries
21.3.1 Injury Rate
Most of the data on injuries is from retrospective studies based on questionnaires or from medical records collected for other purposes. This makes it prone to different limitations (including recall bias or underestimation of minor injuries) and potentially leads to imprecise epidemiological evaluations [13]. Taking into account these considerations, the available data as a whole nevertheless allows us to draw a general risk profile of the sport (Table 21.1
).
Table 21.1
Windsurfing injury rates according to different studies
Study | Population | Total number of participants | Type of data | Injury rate |
|---|---|---|---|---|
McCormick and Davis (1988) [14] | Enthusiasts including the “hurricane sailors” of Galveston Bay, Texas, in the Gulf of Mexico | 73 | Hospital medical records and questionnaire interviews | 0.22/1000 windsurfing hours |
Mettler and Biener (1991) [15] | Members of the Swiss Windsurfing Federation | 189 | Medical history | 0.02 injuries/athlete/year |
Salvi et al. (1997) [16] | National and international competition windsurfers taking part in the 1993 Italian Championship | 123 | Medical history | 0.003 injuries/athlete/year 0.22/1000 windsurfing hours |
Nathanson and Reinert (1999) [13] | Predominantly amateurs (99.3 %), practicing in the United States and the Dominican Republic, and recruited via the Internet | 294 | Specific questionnaire | 0.36/1000 windsurfing hours |
Prymka et al. (1999) [17] | Competitors in the German Windsurfing Cup 1995 | 44 | Specific questionnaire | 2.04/person/year (extrapolated) |
Petersen et al. (2003) [18] | Recreational (72 %), competitors (20 %), and beginner (8 %) German windsurfers in the 2000 season | 327 | Specific questionnaire | 1.92/participant/year (extrapolated) |
Dyson et al. (2006) [19] | Race board national/international competitors (33.6 %), wave/slalom national/international competitors (40.2 %), and recreational windsurfers (26.2 %) in the 1999/2000 seasons | 107 | Specific questionnaire | 1.5/person/year |
Kristen et al. (2007) [20] | Participants in the Windsurf Freestyle World Cup/Euro-Cup during the period 1997–2007, Neusiedl, Austria | 27 (average) | Sports medical records | 0.69/athlete/year (extrapolated) |
According to the relevant literature, acute injuries range between 69 and 78 % of all windsurfing injuries [13, 21]. With respect to injury distribution, lower limbs are the part of the body most commonly affected (Table 21.2
). Most injuries are lacerations or puncture wounds due to contact with equipment and the sea floor and sprains or fractures due to the foot straps.
Table 21.2
Anatomical distribution of injuries according to different studies
Authors | Total number of injuries | Head/neck (%) | Trunk (%) | Upper limbs (%) | Lower limbs (%) |
|---|---|---|---|---|---|
Nathanson and Reinert (1999) [13] | 339 | 17.8 | 16 | 18.5 | 44.6 |
Prymka et al. (1999) [17] | 25 | 16 | 8 | 20 | 56 |
Kristen et al. (2007) [20] | 188 | 26 | 19 | 6 | 38 |
Gosheger et al. (2001) [22] | 260 | 17 | 15 | 9 | 59 |
Hopkins and Hooker (2002) [23] | 222 | 25 | 9 | 8 | 48 |
In the series by Nathanson and Reinert [13], out of 339 acute injuries, the foot was the most common site of acute injury (17.7 %; n = 65), followed by the knee (9.4 %; n = 32), and the ankle (8.6 %; n = 29). Foot injuries were mainly lacerations (48 %; n = 31), while more than half (57 %; n = 35) of knee and ankle injuries considered together were sprains. The upper limbs were the second most affected area of the body (18.5 %; n = 62) with ligamentous injuries and sprains (55 %; n = 34) and shoulder dislocations (15 %; n = 9). Head injuries mainly consisted of contusions (4.7 %; n = 16), while injuries to the trunk were mostly chest wall contusions and rib fractures (8.2 %; n = 28) and back strains or intervertebral disk injuries (4.7 %; n = 16).
A similar injury pattern was found in competitors and elite windsurfers. In a study on 49 professional World Cup windsurfers, Gosheger et al. [22] found ankle strains to be the most common injuries (22 %; n = 57). Knee injuries were also frequent (11.5 %; n = 30). In the study by Kristen et al. [20] examining the Windsurf Freestyle World Cup/Euro-Cup regattas on Lake Neusiedl in Austria between 1997 and 2007, the most common injuries were as follows: sprains and ligament tears to the ankle and foot (18 %; n = 34); acute back pain (17 %; n = 32); head contusions (12.8 %; n = 24); cuts to the feet (11 %; n = 21); and knee injuries (9 %; n = 17). In their study on elite women windsurfers participating in the 2008 PWA World Cup in Fuerteventura in the Canary Islands, Penichet-Tomás et al. [24] found that knees and legs were the most common regions to be affected by injuries in slalom and freestyle respectively. In the series by Dyson et al. [19], muscle/tendon strains accounted for 45 % of new injuries, and acute soft tissue injuries were equally distributed in the upper (n = 129) and lower body (n = 133). Especially in the upper body, most of the injuries affected the shoulder, the upper arm, and the elbow complex (41 %), while 60 % of lower body soft tissue injuries were most frequently related to the knee or the lower leg, the ankle and foot. Finally, in the same study, serious bruising, cuts and abrasions (mainly involving the head and face, the leg and foot regions) were more common especially among wave and slalom.
Although most injuries sustained during windsurfing are minor (sprains, muscle strains, bruises and cuts [12, 13, 18–20]), more serious injuries may occur when windsurfing is practiced in extreme wind and wave conditions or when simple safety rules and procedures are not followed [25]. Kalogeromitros et al. [25] monitored all serious windsurfing incidents in the Aegean Sea during 1999 and reported 22 windsurfing injuries requiring hospitalization at a tertiary level center. These included two cases of drowning, three concussions (one serious enough to require mechanical ventilatory support for 24 h), and a young windsurfer who suffered a C2 fracture resulting in tetraplegia associated with tracheal obstruction requiring emergency tracheotomy.
21.3.2 Causes of Acute Injuries
Collision with equipment when overpowered by wind and waves is the most common cause of trauma [18]. This is the cause in 65–75 % of all injuries [13, 15], the majority of which are caused by the boom, mast and board [13, 23]. In the series by Nathanson and Reinert [13], more than one third of lacerations to the lower limbs were caused by the surfer striking the fin of the board while attempting to waterstart with long narrow “blade” fins causing significantly more injuries (68.5 %; n = 13) than swept-back wave-type fins (31.5 %; n = 6).
According to Fehske et al. [12], 22.3 % of injury events had an external cause such as collisions with kitesurfers or other watercraft. These were not considered as common causes of injury in other studies [12, 13]. According to Nathanson and Reinert [13], the impact with water and contact with the seafloor and marine animals were other important causes of injuries accounting for 12.1 % of the total when taken together. Reports of shark attacks on windsurfers are extremely rare [26]. A greater danger in tropical waters is posed by flying fish which can cause cuts, while collisions with marine turtles can be avoided by paying attention to the fairway [20].
Most injury events occur after 2 h of exercise. This may be caused by fatigue interfering with the proper execution of maneuvers [19]. Broken equipment was reported as a cause of injury in just 3 % (n = 10) of cases (Peterson et al. [18]).
21.3.3 Injury Dynamics
According to Nathanson and Reinert [13], uncontrolled falls represent the most common injury dynamic resulting in more than one third of injuries.
Low-speed falls mainly lead to lower limb injuries ascribed to the pattern of “foot strap injuries”(Fig. 21.3

), while high-speed falls may cause shoulder and head injuries consistent with the mechanism of “catapulting”[13]. The latter occurs when sailors are unable to detach the harness quickly enough causing them to be launched into the air and often land on the mast or the boom. Anterior shoulder dislocations are usually caused by the boardsailor hanging onto the boom while falling. Falls can also lead to head injuries ranging from minor results such as hearing problems and tinnitus to severe concussion with loss of consciousness [25]. In the study by Nathanson and Reinert [13], jumping was the maneuver that most often led to injuries (21 %; n = 71), while launching, jibing, and waterstarting caused 9.4, 7, and 5.9 % of injuries respectively (Fig. 21.4

)
Fig. 21.3
A windsurfer photographed just before a fall caused by miscalculation of the ratio between sailing speed and wave size. The sail is clearly deflated with the low wind pressure giving no potential for recovery. The breaking wave may complicate the fall resulting in dynamic a high-risk for foot strap injuries (Photo: Claudio Marosa)
Fig. 21.4
One-handed jump (Photo: Claudio Marosa)
Since even the most extreme athletes spend less than 5 % of their windsurfing time jumping, this maneuver contributes to a disproportionately high number of injuries. Jumping, looping, and catapult falls also tend to cause injuries requiring medical treatment [13]. In addition, jumps involving rotations of the board and the athlete on both horizontal and vertical planes such as forward and backward looping are the most dangerous maneuvers (Fig. 21.5) [18]. While the consequences of the collisions with kitesurfers or other watercraft are generally absent or minimal, given that windsurfers can reach speeds of 30–60 km/h, potential outcomes include major injuries such as blunt trauma from the board top, craniocerebral trauma and cuts from the fin [20]. Collisions are especially common in the most popular windsurfing spots near cities, often crowded with windsurfers, kiters, and sailors especially during weekends, and they are caused by lack of concentration, ignorance or disregard of the right of way, and high-risk maneuvers [20]. Meteorological conditions, particularly strong winds and large waves [14], may also lead to incidents (Fig. 21.6), especially when weather conditions are unexpected or underestimated [18, 19].


Fig. 21.5
Landing from a push loop (Photo: Claudio Marosa)
Fig. 21.6
A dangerous situation: a fallen windsurfer in large breakers (Photo: Claudio Marosa)
21.4 Acute Injuries Specific to Windsurfing
21.4.1 Foot Strap Injuries
The category of injuries referred to as “foot strap injuries” [22] is specific to windsurfing [16, 28] and represents the vast majority (75 %) of lower limb fractures and ligament injuries [13] involving the ankle, knee or foot. They occur during unexpected falls or a bad landing after a jump and are caused by the disproportionate rotational forces exerted on the lower limbs by the long lever arm of the board when the foot is wedged in the foot strap. This is a mechanism whereby the body twists at the knee on the fixed foreleg possibly causing fractures of the femoral shaft [25], the head of the fibula (Fig. 21.7) and the tibial plateau, as well as knee injuries including dislocations, lesions of the capsule, and tears to the meniscus and collateral and cruciate ligaments [28]. Foot and ankle injuries may also occur when the foot inserted in the foot strap is acutely pronated due to a bad landing or a fall. These include Lisfranc injuries; unusual in other sports, but potentially frequent in windsurfing [36].
Fig. 21.7
Foot strap injury: distal fracture of the fibula, diagnosis, and treatment. Radiographs: anteroposterior (a) and laterolateral (b) projections. showing fracture (indicated by an arrow). Radiographs in the same projections, showing the reduction achieved using a plate, metal screws and plaster splint [1]
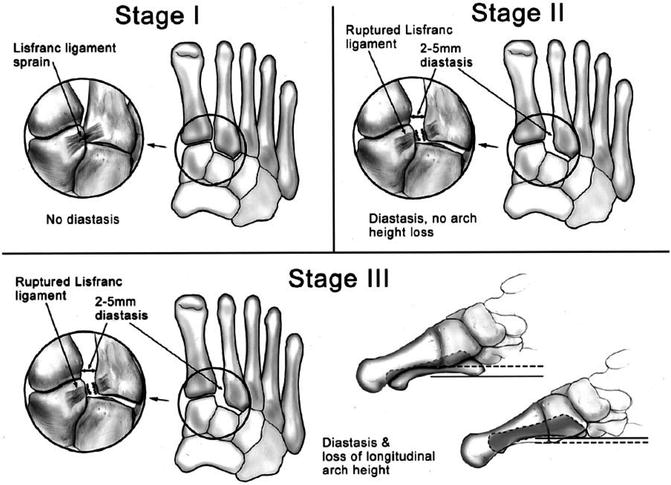
The term Lisfranc injury refers to a wide spectrum of injuries including lesions to the bases of the metatarsals, the four distal tarsal bones and the Lisfranc ligament. The tarsometatarsal joint complex (also referred to as the Lisfranc joint) is architecturally shaped like a “Roman arch” with the base of the second metatarsal acting as its keystone. It is located proximally with respect to the other metatarsal bases, tightly recessed between the first and third cuneiforms in a mortise configuration. The Lisfranc ligament is a strong oblique ligament arising from the plantar-lateral surface of the medial cuneiform to insert on to the plantar medial aspect of the second metatarsal. The traumatic mechanism of these injuries usually involves excessive plantar flexion and abduction of the forefoot often associated with concurrent rotational, compressive, and translative forces [29].
A high level of vigilance is required when evaluating windsurfers who suffer from injuries stemming from this dynamic since delayed diagnosis may lead to post-traumatic arthritis. On examination, anterior foot pain may be associated with ecchymosis or edema of variable entity. In Lisfranc ligament injuries, pain is elicited by moving the first and second metatarsals in opposite directions or by passive abduction and pronation of the forefoot while holding the hindfoot in a fixed position. Plain radiography should be completed with an anterior-posterior weightbearing view and may allow the physician to detect the following signs: misalignment of the medial border of the second metatarsal with the medial margin of the middle cuneiform; diastasis between the first cuneiform and the second metatarsal base; and a small bony fragment between the base of the first and second metatarsal (fleck sign). CT and MRI are more reliable. MRI in particular may show ligament edema as an increased signal on T2-weighted sequences in the case of a strain or ligament discontinuity in the case of a tear, or fractures of the metatarsal bases and tarsal bones, while bone marrow edema within the inferior aspect of the middle cuneiform should be considered a secondary sign of ligament injury. CT is more sensitive to bone injuries allowing a better visualization of these fractures and aiding preoperative planning [28, 31].
Although the best approach to Lisfranc injuries is still debated, stage I (according to Nunley and Vertullo [32], Fig. 21.8) can be non-surgically managed by a non-weightbearing cast for 6–10 weeks with the majority of patients returning to their pre-injury sport activities. With regard to stage II and III injuries, most authors agree that the best treatment strategy involves prompt surgical intervention with anatomic reduction and fixation [32–35]. Despite this, Mitani et al. [36] reported the case of a 40-year-old professional female windsurfer who sustained a Lisfranc injury with a diastasis of more than 3 mm that was treated conservatively. Undeterred by the recommendation for surgical treatment, she was adamant in her preference for non-surgical management. Given that she was close to the late stages of her professional career, a long rest and rehabilitation period required by a surgical approach would have hastened her retirement. The conservative approach was possible because her specialty was racing which is much less demanding compared to wave riding and freestyle in terms of forefoot stresses in the foot straps, A special cork insole mounted inside a marine boot was adopted to support the longitudinal and lateral arch of the foot during windsurfing even when in the strap.