24. Urinary tract infections




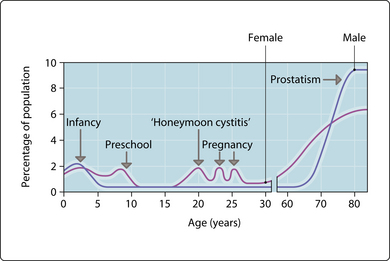
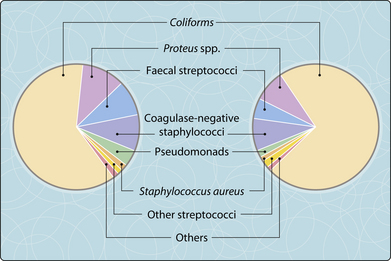
Urinary tract infections (UTI) are more common at certain ages (Fig. 3.24.1). While many infections are mild, renal infections may lead to long-term kidney damage, and the urinary tract is a common source of life-threatening Gram-negative bacteraemia. Risk factors for UTI in infants and children are anatomical and functional anomalies (e.g. ureteric reflux, strictures, neurogenic bladder). Women have a shorter urethra than men and so are more prone to bladder infection, particularly after intercourse. Any obstruction to urine flow can predispose to infection. In pregnancy, the ureter is dilated and can be obstructed by the gravid uterus. In elderly men, prostate enlargement obstructs the urethra and in elderly women a cystocele can lead to residual urine volumes in the bladder. Catheterization introduces exogenous flora, which in hospital are often multiresistant. Figure 3.24.2 shows the likely infecting species in the hospital setting and in the community.
Clinical features
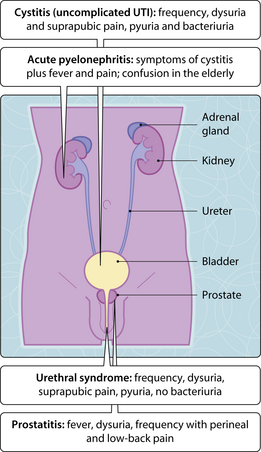
Several clinical syndromes are recognized (Fig. 3.24.3). If women present with dysuria, frequency and suprapubic pain, the probability of uncomplicated UTI is high. If fewer symptoms are present, the urethral syndrome is possible, which is a lower UTI without ‘significant bacteriuria’. The aetiology of this condition is controversial but chlamydial infections may play a role. Asymptomatic bacteriuria (bacteriuria > 105 colony-forming units (CFU)/ml in the absence of pyuria) occurs in approximately 5% of women and is important in pregnancy, where 20–30% will develop acute pyelonephritis if untreated. Bacteriuria in pregnancy is also associated with premature birth, low birthweight and increased perinatal mortality. It is, therefore, important that all women have their urine cultured early in pregnancy.
< div class='tao-gold-member'>
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


